

Effect of health information exchange on recognition of medication discrepancies is interrupted when data charges are introduced: results of a cluster-randomized controlled trial
- PMID: 28505367
- PMCID: PMC7651981
- DOI: 10.1093/jamia/ocx044
Effect of health information exchange on recognition of medication discrepancies is interrupted when data charges are introduced: results of a cluster-randomized controlled trial
Abstract
Objectives: To determine the effect of health information exchange (HIE) on medication prescribing for hospital inpatients in a cluster-randomized controlled trial, and to examine the prescribing effect of availability of information from a large pharmacy insurance plan in a natural experiment.
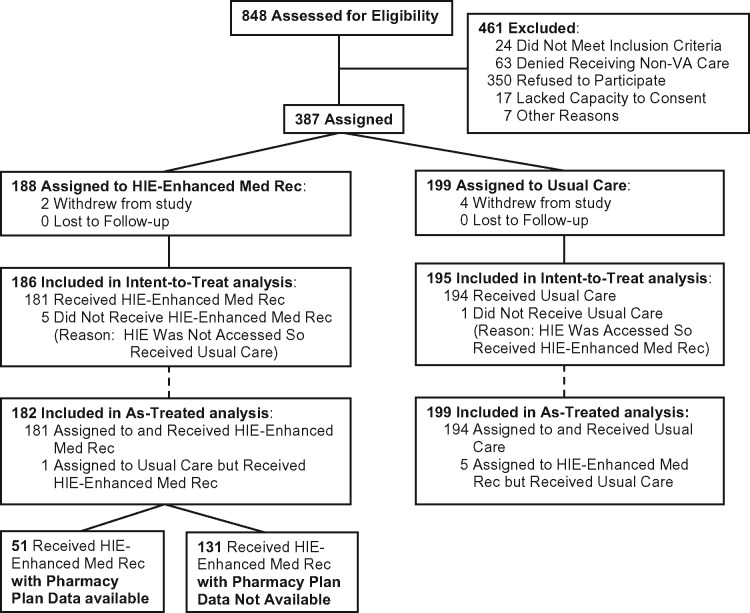
Methods: Patients admitted to an urban hospital received structured medication reconciliation by an intervention pharmacist with (intervention) or without (control) access to a regional HIE. The HIE contained prescribing information from the largest hospitals and pharmacy insurance plan in the region for the first 10 months of the study, but only from the hospitals for the last 21 months, when data charges were imposed by the insurance plan. The primary endpoint was discrepancies between preadmission and inpatient medication regimens, and secondary endpoints included adverse drug events (ADEs) and proportions of rectified discrepancies.
Results: Overall, 186 and 195 patients were assigned to intervention and control, respectively. Patients were 60 years old on average and took a mean of 7 medications before admission. There was no difference between intervention and control in number of risk-weighted discrepancies (6.4 vs 5.8, P = .452), discrepancy-associated ADEs (0.102 vs 0.092 per admission, P = .964), or rectification of discrepancies (0.026 vs 0.036 per opportunity, P = .539). However, patients who received medication reconciliation with pharmacy insurance data available had more risk-weighted medication discrepancies identified than those who received usual care (8.0 vs 5.9, P = .038).
Discussion and conclusion: HIE may improve outcomes of medication reconciliation. Charging for access to medication information interrupts this effect. Efforts are needed to understand and increase prescribers' rectification of medication discrepancies.
Keywords: health information exchange; medication reconciliation; randomized controlled trial.
Published by Oxford University Press on behalf of the American Medical Informatics Association 2017. This work is written by US Government employees and is in the public domain in the United States.
References
-
- Cornish PL, Knowles SR, Marchesano R. et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;1654:424–29. - PubMed
-
- Boockvar K, Fishman E, Kyriacou CK. et al. Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med. 2004;1645:545–50. - PubMed
-
- Johnson JA, Bootman JL. Drug-related morbidity and mortality. A cost-of-illness model. Arch Intern Med. 1995;15518:1949–56. - PubMed
-
- Boockvar KS, Blum S, Kugler A. et al. Effect of admission medication reconciliation on adverse drug events from admission medication changes. Arch Intern Med. 2011;1719:860–61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
