

A Short and Distinct Time Window for Recovery of Arm Motor Control Early After Stroke Revealed With a Global Measure of Trajectory Kinematics
- PMID: 28506149
- PMCID: PMC5434710
- DOI: 10.1177/1545968317697034
A Short and Distinct Time Window for Recovery of Arm Motor Control Early After Stroke Revealed With a Global Measure of Trajectory Kinematics
Abstract
Background: Studies demonstrate that most arm motor recovery occurs within three months after stroke, when measured with standard clinical scales. Improvements on these measures, however, reflect a combination of recovery in motor control, increases in strength, and acquisition of compensatory strategies.
Objective: To isolate and characterize the time course of recovery of arm motor control over the first year poststroke.
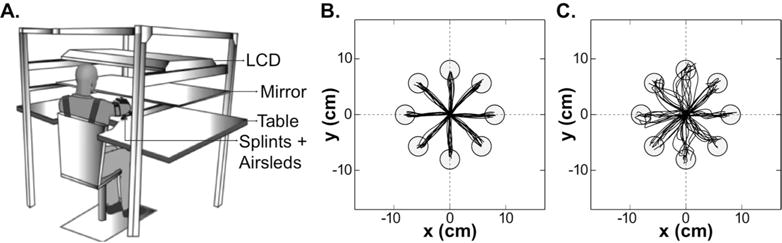
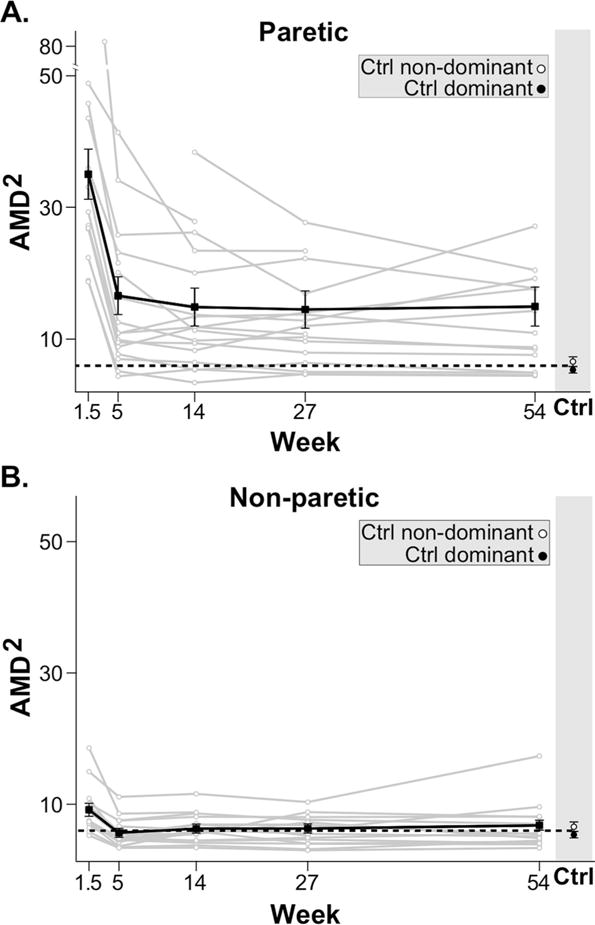
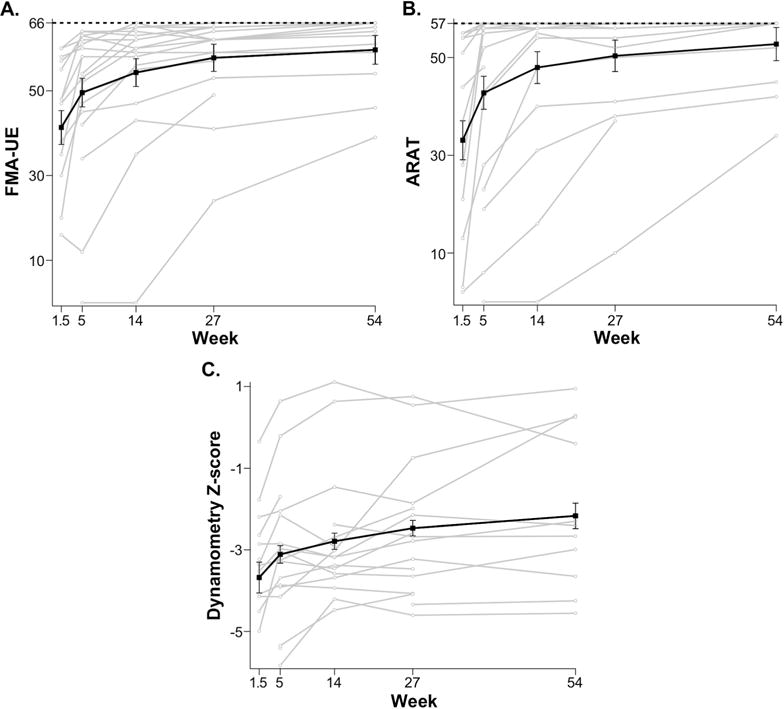
Methods: Longitudinal study of 18 participants with acute ischemic stroke. Motor control was evaluated using a global kinematic measure derived from a 2-dimensional reaching task designed to minimize the need for antigravity strength and prevent compensation. Arm impairment was evaluated with the Fugl-Meyer Assessment of the upper extremity (FMA-UE), activity limitation with the Action Research Arm Test (ARAT), and strength with biceps dynamometry. Assessments were conducted at: 1.5, 5, 14, 27, and 54 weeks poststroke.
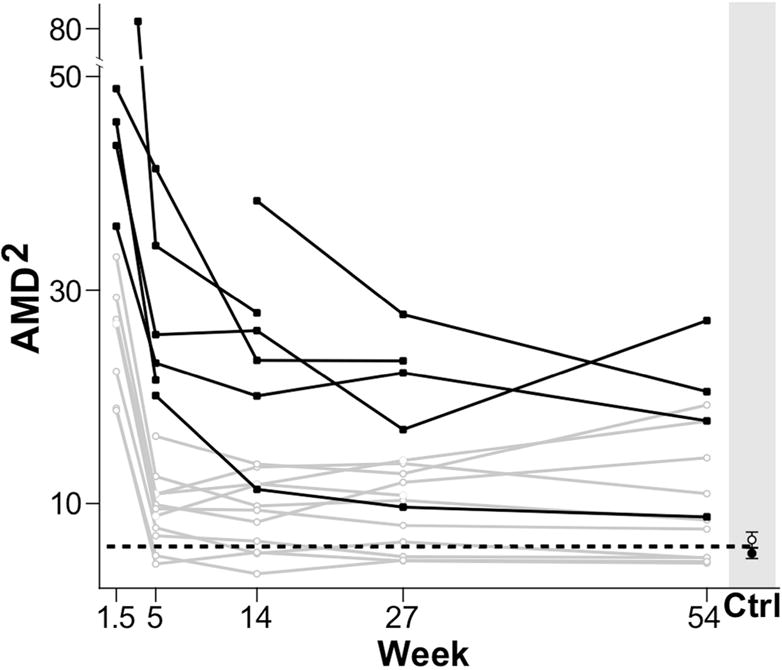
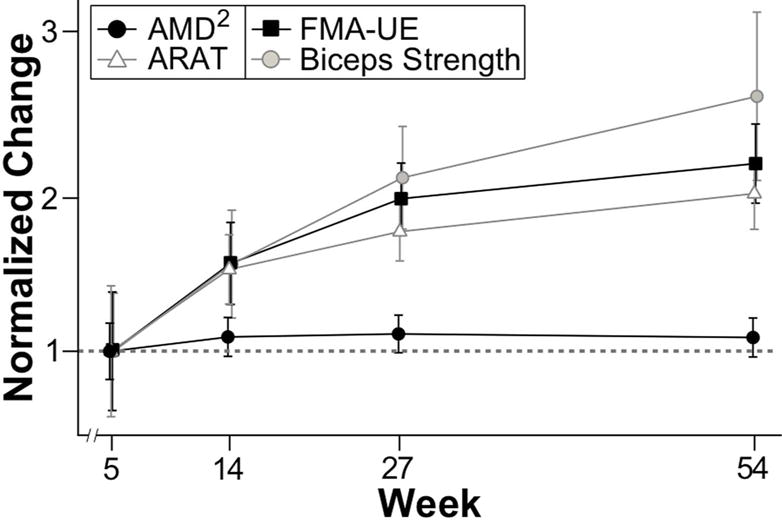
Results: Motor control in the paretic arm improved up to week 5, with no further improvement beyond this time point. In contrast, improvements in the FMA-UE, ARAT, and biceps dynamometry continued beyond 5 weeks, with a similar magnitude of improvement between weeks 5 and 54 as the one observed between weeks 1.5 and 5.
Conclusions: Recovery after stroke plateaued much earlier for arm motor control, isolated with a global kinematic measure, compared to motor function assessed with clinical scales. This dissociation between the time courses of kinematic and clinical measures of recovery may be due to the contribution of strength improvement to the latter. Novel interventions, focused on the first month poststroke, will be required to exploit the narrower window of spontaneous recovery for motor control.
Keywords: kinematics; motor recovery; reaching; stroke; upper limb.
Figures
References
-
- World Health Organization. Towards a common language for functioning, disability and health. ICF; 2002.
-
- Rathore SS, Hinn AR, Cooper LS, Tyroler HA, Rosamond WD. Characterization of incident stroke signs and symptoms. Stroke; a journal of cerebral circulation. 2002;33(11):2718–2721. 2002/11/01/ - PubMed
-
- Duncan PW, Goldstein LB, Matchar D, Divine GW, Feussner J. Measurement of motor recovery after stroke. Outcome assessment and sample size requirements. Stroke; a journal of cerebral circulation. 1992;23(8):1084–1089. 1992/08/01/ - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
