

Changes in microbial ecology after fecal microbiota transplantation for recurrent C. difficile infection affected by underlying inflammatory bowel disease
- PMID: 28506317
- PMCID: PMC5433077
- DOI: 10.1186/s40168-017-0269-3
Changes in microbial ecology after fecal microbiota transplantation for recurrent C. difficile infection affected by underlying inflammatory bowel disease
Abstract
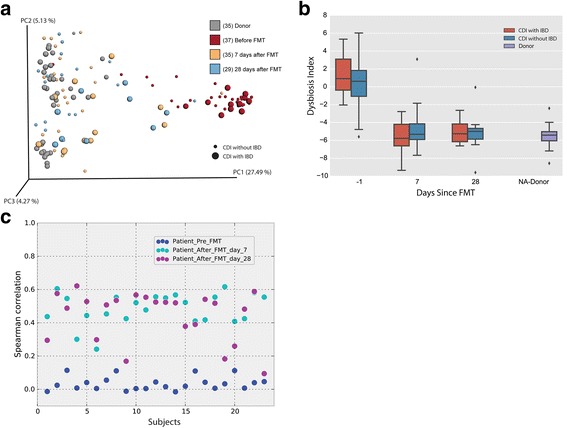
Background: Gut microbiota play a key role in maintaining homeostasis in the human gut. Alterations in the gut microbial ecosystem predispose to Clostridium difficile infection (CDI) and gut inflammatory disorders such as inflammatory bowel disease (IBD). Fecal microbiota transplantation (FMT) from a healthy donor can restore gut microbial diversity and pathogen colonization resistance; consequently, it is now being investigated for its ability to improve inflammatory gut conditions such as IBD. In this study, we investigated changes in gut microbiota following FMT in 38 patients with CDI with or without underlying IBD.
Results: There was a significant change in gut microbial composition towards the donor microbiota and an overall increase in microbial diversity consistent with previous studies after FMT. FMT was successful in treating CDI using a diverse set of donors, and varying degrees of donor stool engraftment suggesting that donor type and degree of engraftment are not drivers of a successful FMT treatment of CDI. However, patients with underlying IBD experienced an increased number of CDI relapses (during a 24-month follow-up) and a decreased growth of new taxa, as compared to the subjects without IBD. Moreover, the need for IBD therapy did not change following FMT. These results underscore the importance of the existing gut microbial landscape as a decisive factor to successfully treat CDI and potentially for improvement of the underlying pathophysiology in IBD.
Conclusions: FMT leads to a significant change in microbial diversity in patients with recurrent CDI and complete resolution of symptoms. Stool donor type (related or unrelated) and degree of engraftment are not the key for successful treatment of CDI by FMT. However, CDI patients with IBD have higher proportion of the original community after FMT and lack of improvement of their IBD symptoms and increased episodes of CDI on long-term follow-up.
Keywords: Clostridium difficile infection; Fecal microbiota transplantation; Inflammatory bowel disease; Microbiome.
Figures

References
-
- Khanna S, Pardi DS. Clinical implications of antibiotic impact on gastrointestinal microbiota and Clostridium difficile infection. Expert Rev Gastroenterol Hepatol. 2016;1–8. [Epub ahead of print]. - PubMed
-
- Orenstein R, Dubberke E, Hardi R, Ray A, Mullane K, Pardi DS, Ramesh MS, Investigators PC. Safety and durability of RBX2660 (microbiota suspension) for recurrent Clostridium difficile infection: results of the PUNCH CD study. Clin Infect Dis. 2016;62(5):596–602. doi: 10.1093/cid/civ938. - DOI - PubMed
-
- Khanna S, Pardi DS, Kelly CR, Kraft CS, Dhere T, Henn MR, Lombardo MJ, Vulic M, Ohsumi T, Winkler J et al. A novel microbiome therapeutic increases gut microbial diversity and prevents recurrent Clostridium difficile infection. J Infect Dis. 2016. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
