

Autonomic dysreflexia after spinal cord injury: Systemic pathophysiology and methods of management
- PMID: 28506502
- PMCID: PMC5677594
- DOI: 10.1016/j.autneu.2017.05.002
Autonomic dysreflexia after spinal cord injury: Systemic pathophysiology and methods of management
Abstract
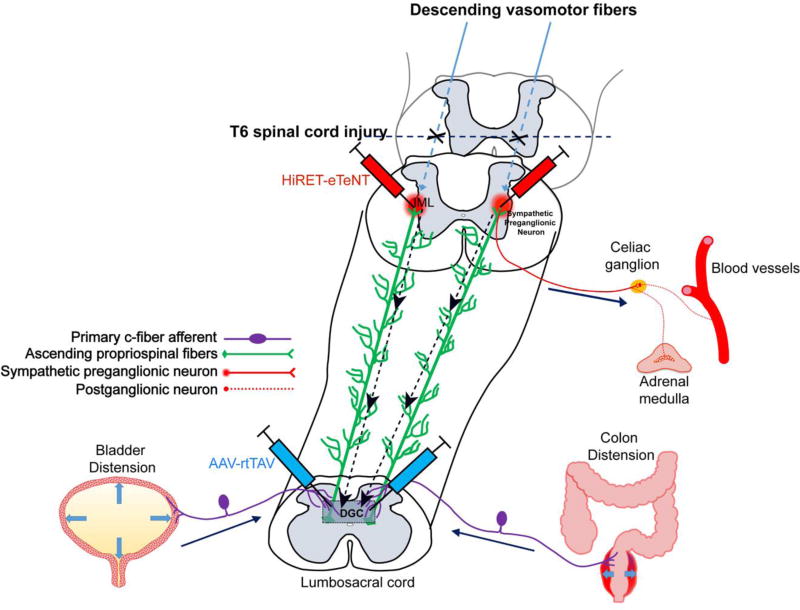
Traumatic spinal cord injury (SCI) has widespread physiological effects beyond the disruption of sensory and motor function, notably the loss of normal autonomic and cardiovascular control. Injury at or above the sixth thoracic spinal cord segment segregates critical spinal sympathetic neurons from supraspinal modulation which can result in a syndrome known as autonomic dysreflexia (AD). AD is defined as episodic hypertension and concomitant baroreflex-mediated bradycardia initiated by unmodulated sympathetic reflexes in the decentralized cord. This condition is often triggered by noxious yet unperceived visceral or somatic stimuli below the injury level and if severe enough can require immediate medical attention. Herein, we review the pathophysiological mechanisms germane to the development of AD, including maladaptive plasticity of neural circuits mediating abnormal sympathetic reflexes and hypersensitization of peripheral vasculature that collectively contribute to abnormal hemodynamics after SCI. Further, we discuss the systemic effects of recurrent AD and pharmacological treatments used to manage such episodes. Contemporary research avenues are then presented to better understand the relative contributions of underlying mechanisms and to elucidate the effects of recurring AD on cardiovascular and immune functions for developing more targeted and effective treatments to attenuate the development of this insidious syndrome following high-level SCI.
Keywords: Hypertension; Maladaptive plasticity; Primary afferent; Propriospinal; Sprouting; Sympathetic.
Copyright © 2017 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Segmental organization of spinal reflexes mediating autonomic dysreflexia after spinal cord injury.Prog Brain Res. 2006;152:265-74. doi: 10.1016/S0079-6123(05)52017-X. Prog Brain Res. 2006. PMID: 16198706 Free PMC article. Review.
-
Intraspinal Plasticity Associated With the Development of Autonomic Dysreflexia After Complete Spinal Cord Injury.Front Cell Neurosci. 2019 Nov 8;13:505. doi: 10.3389/fncel.2019.00505. eCollection 2019. Front Cell Neurosci. 2019. PMID: 31780900 Free PMC article.
-
Autonomic dysreflexia after spinal cord injury: central mechanisms and strategies for prevention.Prog Brain Res. 2006;152:245-63. doi: 10.1016/S0079-6123(05)52016-8. Prog Brain Res. 2006. PMID: 16198705 Review.
-
Soluble TNFα Signaling within the Spinal Cord Contributes to the Development of Autonomic Dysreflexia and Ensuing Vascular and Immune Dysfunction after Spinal Cord Injury.J Neurosci. 2018 Apr 25;38(17):4146-4162. doi: 10.1523/JNEUROSCI.2376-17.2018. Epub 2018 Apr 2. J Neurosci. 2018. PMID: 29610439 Free PMC article.
-
Autonomic dysreflexia and primary afferent sprouting after clip-compression injury of the rat spinal cord.J Neurotrauma. 2001 Oct;18(10):1107-19. doi: 10.1089/08977150152693782. J Neurotrauma. 2001. PMID: 11686496
Cited by
-
Heart rate and blood pressure response improve the prediction of orthostatic cardiovascular dysregulation in persons with chronic spinal cord injury.Physiol Rep. 2020 Oct;8(20):e14617. doi: 10.14814/phy2.14617. Physiol Rep. 2020. PMID: 33080121 Free PMC article.
-
Safety and preliminary efficacy of functional electrical stimulation cycling in an individual with cervical cord injury, autonomic dysreflexia, and a pacemaker: Case report.J Spinal Cord Med. 2021 Jul;44(4):613-616. doi: 10.1080/10790268.2019.1692180. Epub 2019 Dec 6. J Spinal Cord Med. 2021. PMID: 31809247 Free PMC article.
-
Autonomic cardiovascular dysfunction during simple arithmetic test in a patient with cervical spinal cord injury-a case report.Spinal Cord Ser Cases. 2021 Aug 26;7(1):78. doi: 10.1038/s41394-021-00439-w. Spinal Cord Ser Cases. 2021. PMID: 34446698 Free PMC article.
-
Updating perspectives on spinal cord function: motor coordination, timing, relational processing, and memory below the brain.Front Syst Neurosci. 2024 Feb 20;18:1184597. doi: 10.3389/fnsys.2024.1184597. eCollection 2024. Front Syst Neurosci. 2024. PMID: 38444825 Free PMC article. Review.
-
Resveratrol Can Attenuate Astrocyte Activation to Treat Spinal Cord Injury by Inhibiting Inflammatory Responses.Mol Neurobiol. 2021 Nov;58(11):5799-5813. doi: 10.1007/s12035-021-02509-4. Epub 2021 Aug 19. Mol Neurobiol. 2021. PMID: 34410605 Free PMC article. Review.
References
-
- Ackery AD, Norenberg MD, Krassioukov A. Calcitonin gene-related peptide immunoreactivity in chronic human spinal cord injury. Spinal cord. 2007;45:678–686. - PubMed
-
- Al Dera H, Habgood MD, Furness JB, Brock JA. Prominent contribution of L-type Ca2+ channels to cutaneous neurovascular transmission that is revealed after spinal cord injury augments vasoconstriction. Am J Physiol Heart Circ Physiol. 2012;302:H752–762. - PubMed
-
- Al-Chaer ED, Lawand NB, Westlund KN, Willis WD. Pelvic visceral input into the nucleus gracilis is largely mediated by the postsynaptic dorsal column pathway. J Neurophysiol. 1996;76:2675–2690. - PubMed
-
- Alan N, Ramer LM, Inskip JA, Golbidi S, Ramer MS, Laher I, Krassioukov AV. Recurrent autonomic dysreflexia exacerbates vascular dysfunction after spinal cord injury. Spine J. 2010;10:1108–1117. - PubMed
-
- Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. Journal of neurotrauma. 2004;21:1371–1383. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
