

Applying nanomedicine in maladaptive inflammation and angiogenesis
- PMID: 28506745
- PMCID: PMC5682240
- DOI: 10.1016/j.addr.2017.05.009
Applying nanomedicine in maladaptive inflammation and angiogenesis
Abstract
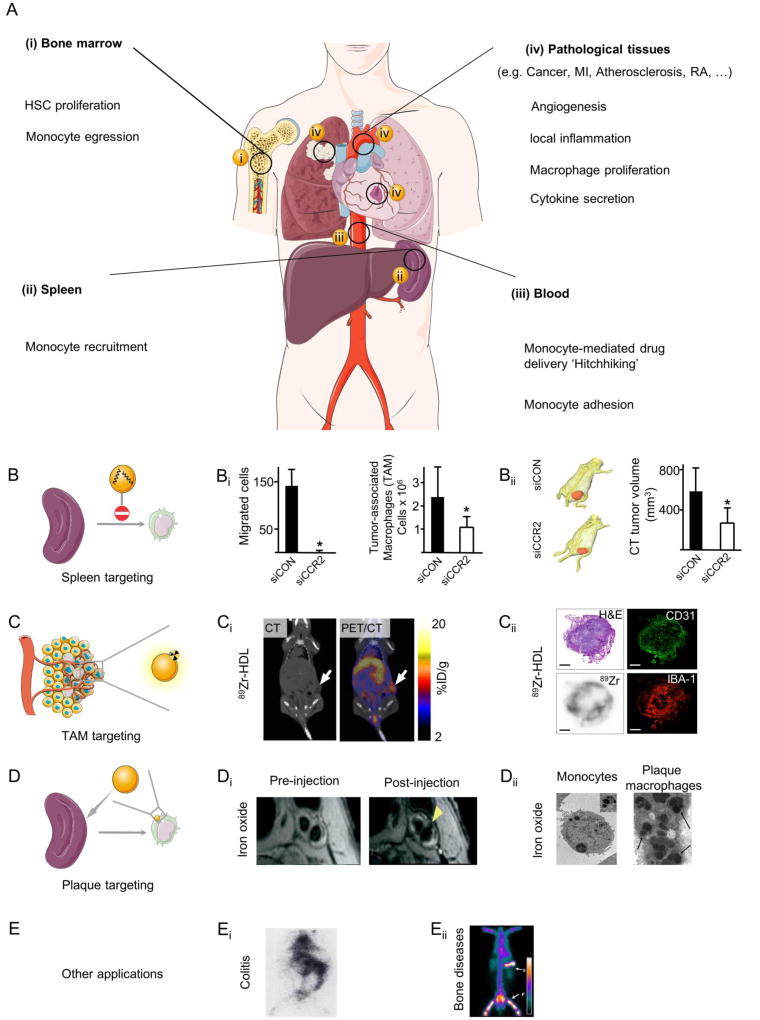
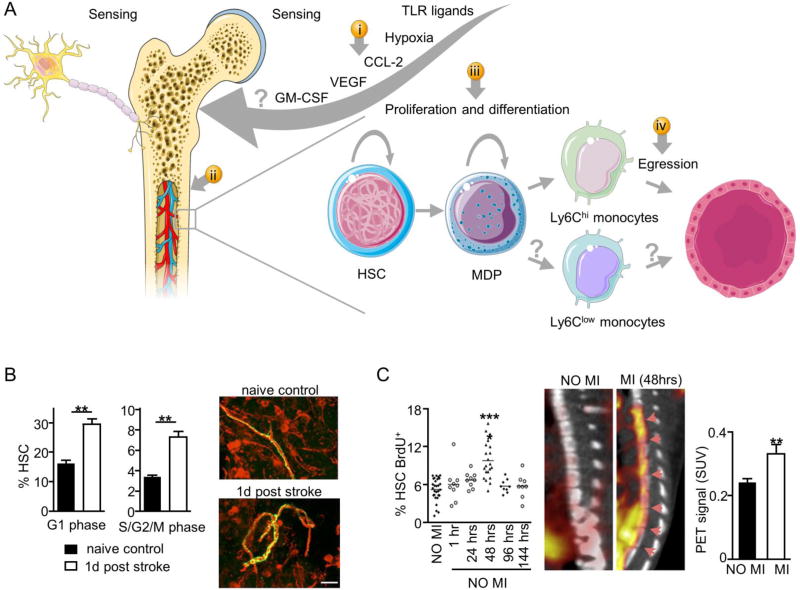
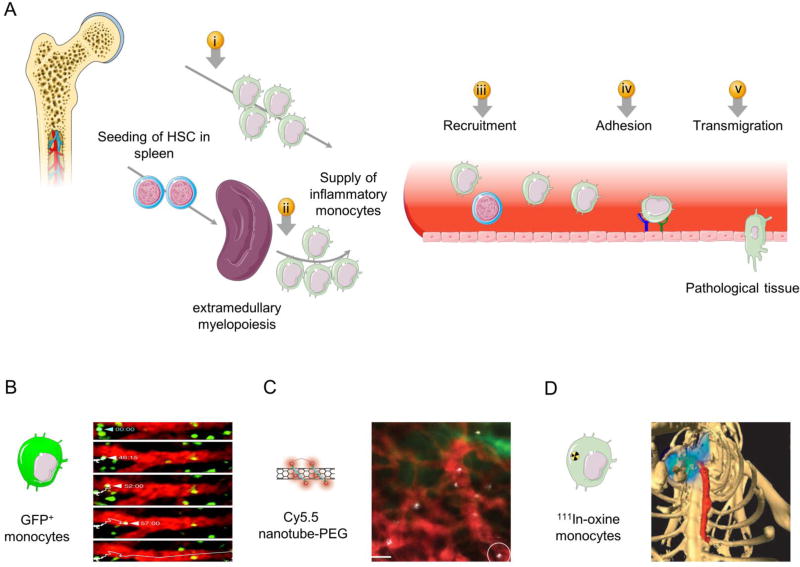
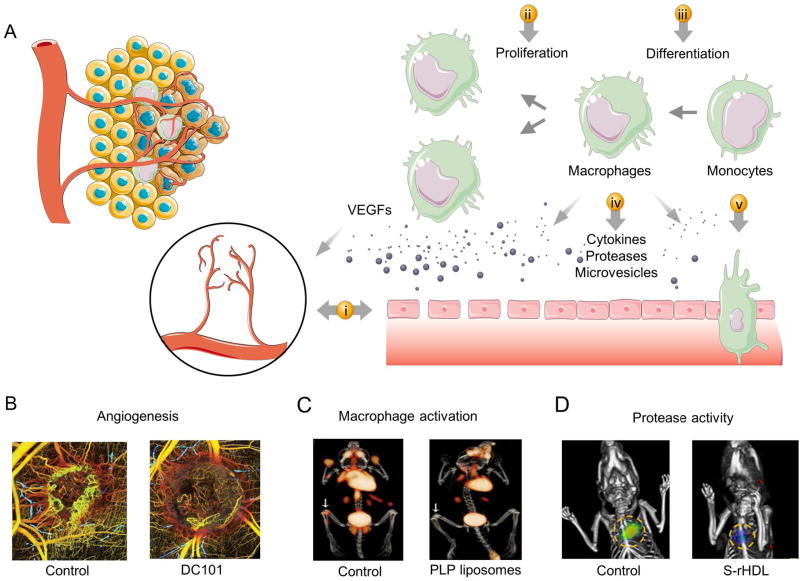
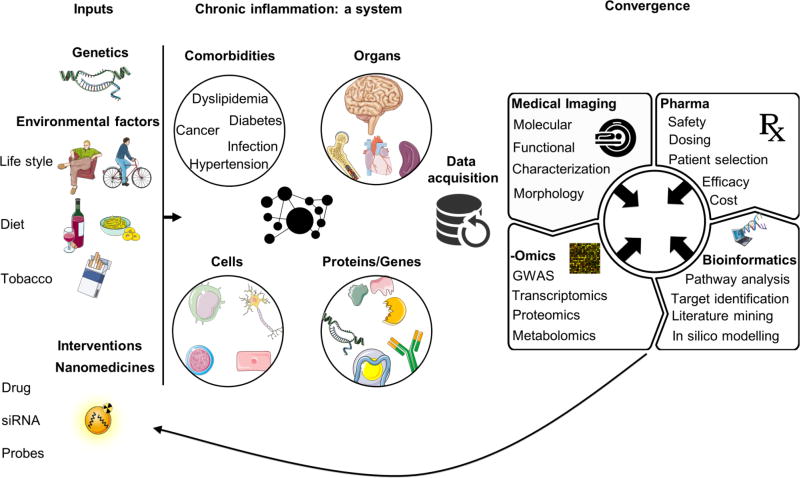
Inflammation and angiogenesis drive the development and progression of multiple devastating diseases such as atherosclerosis, cancer, rheumatoid arthritis, and inflammatory bowel disease. Though these diseases have very different phenotypic consequences, they possess several common pathophysiological features in which monocyte recruitment, macrophage polarization, and enhanced vascular permeability play critical roles. Thus, developing rational targeting strategies tailored to the different stages of the journey of monocytes, from bone marrow to local lesions, and their extravasation from the vasculature in diseased tissues will advance nanomedicine. The integration of in vivo imaging uniquely allows studying nanoparticle kinetics, accumulation, clearance, and biological activity, at levels ranging from subcellular to an entire organism, and will shed light on the fate of intravenously administered nanomedicines. We anticipate that convergence of nanomedicines, biomedical engineering, and life sciences will help to advance clinically relevant therapeutics and diagnostic agents for patients with chronic inflammatory diseases.
Keywords: Angiogenesis; Atherosclerosis; Cancer; Chronic inflammation; Immunomodulation; Macrophages; Molecular imaging; Monocytes; Nanomedicine; Targeted drug delivery.
Copyright © 2017 Elsevier B.V. All rights reserved.
Figures
References
-
- Strong K, Mathers C, Leeder S, Beaglehole R. Preventing chronic diseases: how many lives can we save? Lancet (London, England) 2005;366:1578–1582. doi:S0140-6736(05)67341-2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
