

Patients double-seropositive for ANCA and anti-GBM antibodies have varied renal survival, frequency of relapse, and outcomes compared to single-seropositive patients
- PMID: 28506760
- PMCID: PMC5567410
- DOI: 10.1016/j.kint.2017.03.014
Patients double-seropositive for ANCA and anti-GBM antibodies have varied renal survival, frequency of relapse, and outcomes compared to single-seropositive patients
Abstract
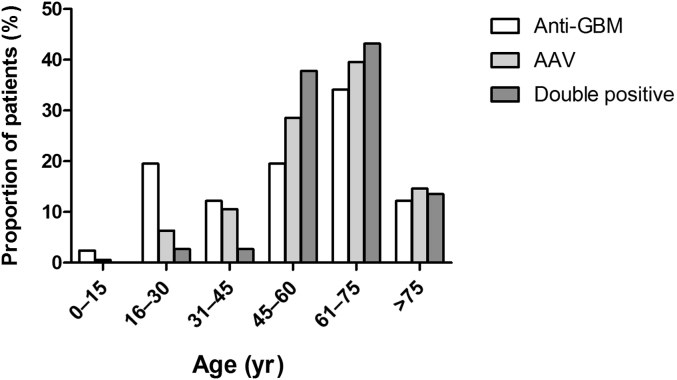
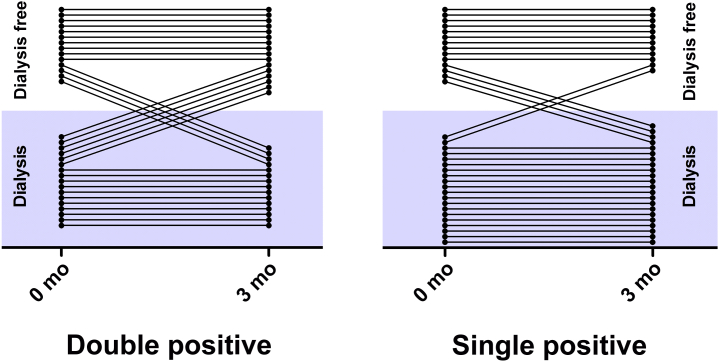
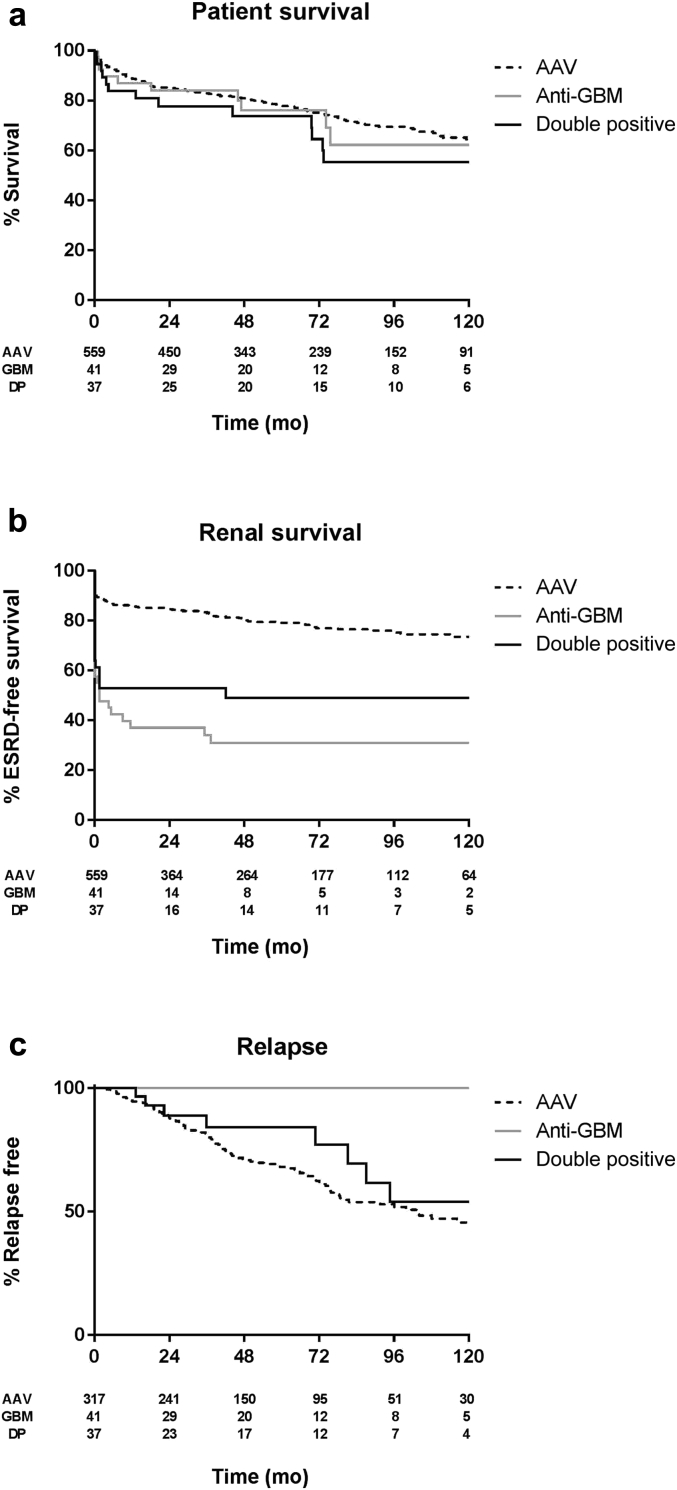
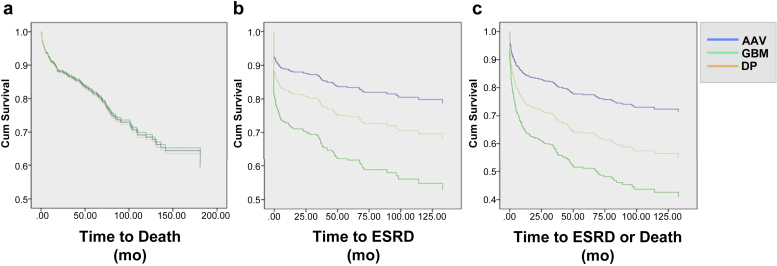
Co-presentation with both ANCA and anti-GBM antibodies is thought to be relatively rare. Current studies of such 'double-positive' cases report small numbers and variable outcomes. To study this further we retrospectively analyzed clinical features and long-term outcomes of a large cohort of 568 contemporary patients with ANCA-associated vasculitis, 41 patients with anti-GBM disease, and 37 double-positive patients with ANCA and anti-GBM disease from four European centers. Double-positive patients shared characteristics of ANCA-associated vasculitis (AAV), such as older age distribution and longer symptom duration before diagnosis, and features of anti-GBM disease, such as severe renal disease and high frequency of lung hemorrhage at presentation. Despite having more evidence of chronic injury on renal biopsy compared to patients with anti-GBM disease, double-positive patients had a greater tendency to recover from being dialysis-dependent after treatment and had intermediate long-term renal survival compared to the single-positive patients. However, overall patient survival was similar in all three groups. Predictors of poor patient survival included advanced age, severe renal failure, and lung hemorrhage at presentation. No single-positive anti-GBM patients experienced disease relapse, whereas approximately half of surviving patients with AAV and double-positive patients had recurrent disease during a median follow-up of 4.8 years. Thus, double-positive patients have a truly hybrid disease phenotype, requiring aggressive early treatment for anti-GBM disease, and careful long-term follow-up and consideration for maintenance immunosuppression for AAV. Since double-positivity appears common, further work is required to define the underlying mechanisms of this association and define optimum treatment strategies.
Keywords: Goodpasture syndrome; anti-GBM disease; anti–neutrophil cytoplasm antibody; glomerulonephritis; vasculitis.
Copyright © 2017 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
ANCA in anti-GBM disease: moving beyond a one-dimensional clinical phenotype.Kidney Int. 2017 Sep;92(3):544-546. doi: 10.1016/j.kint.2017.04.024. Kidney Int. 2017. PMID: 28807260
References
-
- Pusey C.D. Anti-glomerular basement membrane disease. Kidney Int. 2003;64:1535–1550. - PubMed
-
- Watts R.A., Mahr A., Mohammad A.J. Classification, epidemiology and clinical subgrouping of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis. Nephrol Dial Transplant. 2015;30(Suppl 1):i14–i22. - PubMed
-
- O’Donoghue D.J., Short C.D., Brenchley P.E. Sequential development of systemic vasculitis with anti-neutrophil cytoplasmic antibodies complicating anti-glomerular basement membrane disease. Clin Nephrol. 1989;32:251–255. - PubMed
-
- Jayne D.R., Marshall P.D., Jones S.J. Autoantibodies to GBM and neutrophil cytoplasm in rapidly progressive glomerulonephritis. Kidney Int. 1990;37:965–970. - PubMed
-
- Levy J.B., Hammad T., Coulthart A. Clinical features and outcome of patients with both ANCA and anti-GBM antibodies. Kidney Int. 2004;66:1535–1540. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
