

Benefit of Ezetimibe Added to Simvastatin in Reduced Kidney Function
- PMID: 28507057
- PMCID: PMC5619955
- DOI: 10.1681/ASN.2016090957
Benefit of Ezetimibe Added to Simvastatin in Reduced Kidney Function
Abstract
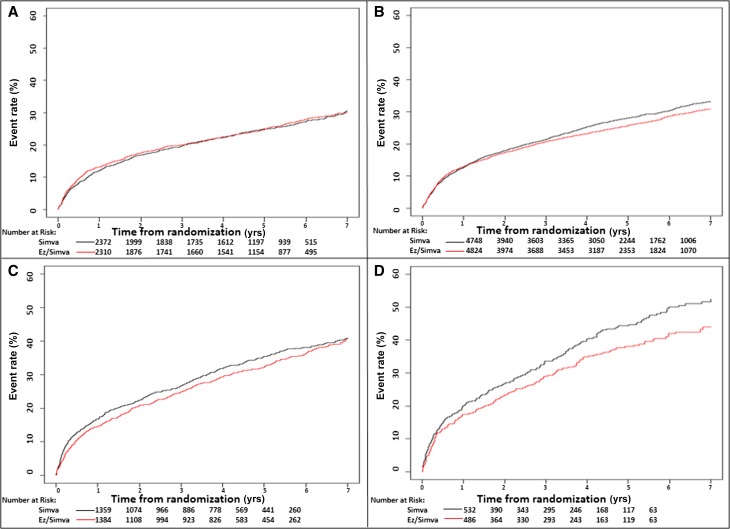
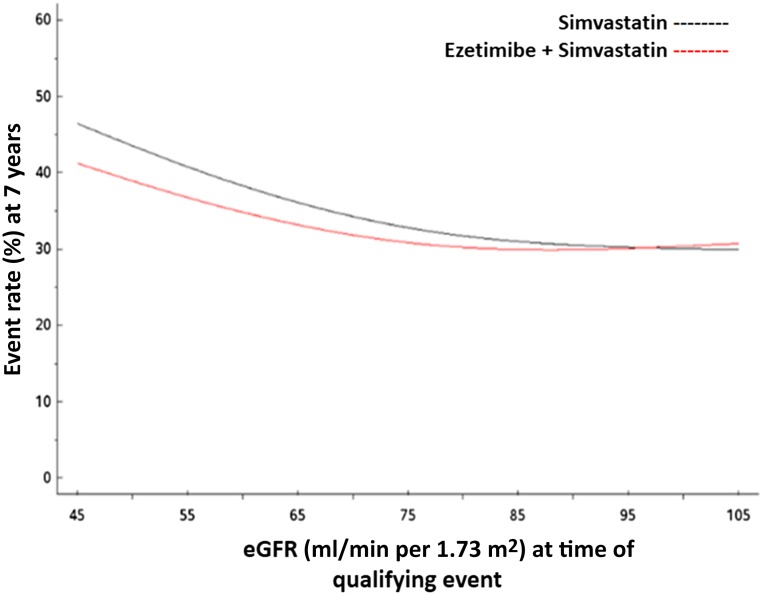
Efficacy of statin-based therapies in reducing cardiovascular mortality in individuals with CKD seems to diminish as eGFR declines. The strongest evidence supporting the cardiovascular benefit of statins in individuals with CKD was shown with ezetimibe plus simvastatin versus placebo. However, whether combination therapy or statin alone resulted in cardiovascular benefit is uncertain. Therefore, we estimated GFR in 18,015 individuals from the IMPROVE-IT (ezetimibe plus simvastatin versus simvastatin alone in individuals with cardiovascular disease and creatinine clearance >30 ml/min) and examined post hoc the relationship of eGFR with end points across treatment arms. For the primary end point of cardiovascular death, major coronary event, or nonfatal stroke, the relative risk reduction of combination therapy compared with monotherapy differed by eGFR (P=0.04). The difference in treatment effect was observed at eGFR≤75 ml/min per 1.73 m2 and most apparent at levels ≤60 ml/min per 1.73 m2 Compared with individuals receiving monotherapy, individuals receiving combination therapy with a baseline eGFR of 60 ml/min per 1.73 m2 experienced a 12% risk reduction (hazard ratio [HR], 0.88; 95% confidence interval [95% CI], 0.82 to 0.95); those with a baseline eGFR of 45 ml/min per 1.73 m2 had a 13% risk reduction (HR, 0.87; 95% CI, 0.78 to 0.98). In stabilized individuals within 10 days of acute coronary syndrome, combination therapy seemed to be more effective than monotherapy in individuals with moderately reduced eGFR (30-60 ml/min per 1.73 m2). Further studies examining potential benefits of combination lipid-lowering therapy in individuals with CKD are needed.
Keywords: cardiovascular; chronic kidney disease; lipids; statins.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, McCullough PA, Kasiske BL, Kelepouris E, Klag MJ, Parfrey P, Pfeffer M, Raij L, Spinosa DJ, Wilson PW; American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention : Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Hypertension 42: 1050–1065, 2003 - PubMed
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Gansevoort RT; Chronic Kidney Disease Prognosis Consortium : Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 375: 2073–2081, 2010 - PMC - PubMed
-
- Fellström BC, Jardine AG, Schmieder RE, Holdaas H, Bannister K, Beutler J, Chae DW, Chevaile A, Cobbe SM, Grönhagen-Riska C, De Lima JJ, Lins R, Mayer G, McMahon AW, Parving HH, Remuzzi G, Samuelsson O, Sonkodi S, Sci D, Süleymanlar G, Tsakiris D, Tesar V, Todorov V, Wiecek A, Wüthrich RP, Gottlow M, Johnsson E, Zannad F; AURORA Study Group : Rosuvastatin and cardiovascular events in patients undergoing hemodialysis. N Engl J Med 360: 1395–1407, 2009 - PubMed
-
- Hou W, Lv J, Perkovic V, Yang L, Zhao N, Jardine MJ, Cass A, Zhang H, Wang H: Effect of statin therapy on cardiovascular and renal outcomes in patients with chronic kidney disease: A systematic review and meta-analysis. Eur Heart J 34: 1807–1817, 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
