

Association between diffuse myocardial fibrosis and diastolic dysfunction in sickle cell anemia
- PMID: 28507082
- PMCID: PMC5510791
- DOI: 10.1182/blood-2017-02-767624
Association between diffuse myocardial fibrosis and diastolic dysfunction in sickle cell anemia
Abstract
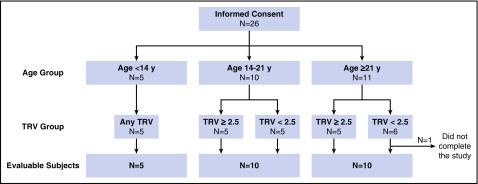
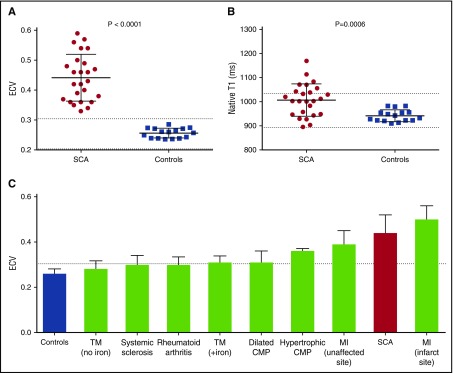
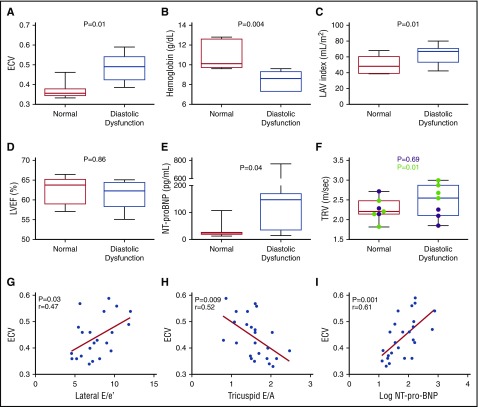
Sickle cell anemia (SCA)-related cardiomyopathy is characterized by diastolic dysfunction and hyperdynamic features. Diastolic dysfunction portends early mortality in SCA. Diastolic dysfunction is associated with microscopic myocardial fibrosis in SCA mice, but the cause of diastolic dysfunction in humans with SCA is unknown. We used cardiac magnetic resonance measurements of extracellular volume fraction (ECV) to discover and quantify diffuse myocardial fibrosis in 25 individuals with SCA (mean age, 23 ± 13 years) and determine the association between diffuse myocardial fibrosis and diastolic dysfunction. ECV was calculated from pre- and post-gadolinium T1 measurements of blood and myocardium, and diastolic function was assessed by echocardiography. ECV was markedly increased in all participants compared with controls (0.44 ± 0.08 vs 0.26 ± 0.02, P < .0001), indicating the presence of diffuse myocardial fibrosis. Seventeen patients (71%) had diastolic abnormalities, and 7 patients (29%) met the definition of diastolic dysfunction. Participants with diastolic dysfunction had higher ECV (0.49 ± 0.07 vs 0.37 ± 0.04, P = .01) and N-terminal pro-brain natriuretic peptide (NT-proBNP; 191 ± 261 vs 33 ± 33 pg/mL, P = .04) but lower hemoglobin (8.4 ± 0.3 vs 10.9 ± 1.4 g/dL, P = .004) compared with participants with normal diastolic function. Participants with the highest ECV values (≥0.40) were more likely to have diastolic dysfunction (P = .003) and increased left atrial volume (57 ± 11 vs 46 ± 12 mL/m2, P = .04) compared with those with ECV <0.4. ECV correlated with hemoglobin (r = -0.46, P = .03) and NT-proBNP (r = 0.62, P = .001). In conclusion, diffuse myocardial fibrosis, determined by ECV, is a common and previously underappreciated feature of SCA that is associated with diastolic dysfunction, anemia, and high NT-proBNP. Diffuse myocardial fibrosis is a novel mechanism that appears to underlie diastolic dysfunction in SCA.
© 2017 by The American Society of Hematology.
Figures
Comment in
-
Myocardial fibrosis: the heart of diastole?Blood. 2017 Jul 13;130(2):104-105. doi: 10.1182/blood-2017-05-786335. Blood. 2017. PMID: 28705857 No abstract available.
References
-
- Machado RF, Anthi A, Steinberg MH, et al. ; MSH Investigators. N-terminal pro-brain natriuretic peptide levels and risk of death in sickle cell disease. JAMA. 2006;296(3):310-318. - PubMed
-
- Gladwin MT, Sachdev V, Jison ML, et al. . Pulmonary hypertension as a risk factor for death in patients with sickle cell disease. N Engl J Med. 2004;350(9):886-895. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
