

Essential information: Uncertainty and optimal control of Ebola outbreaks
- PMID: 28507121
- PMCID: PMC5465899
- DOI: 10.1073/pnas.1617482114
Essential information: Uncertainty and optimal control of Ebola outbreaks
Abstract
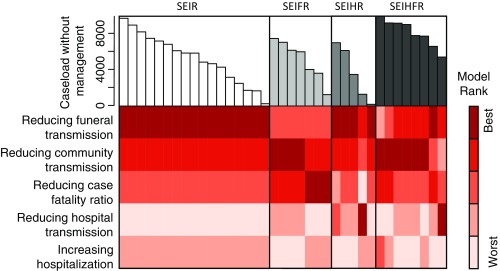
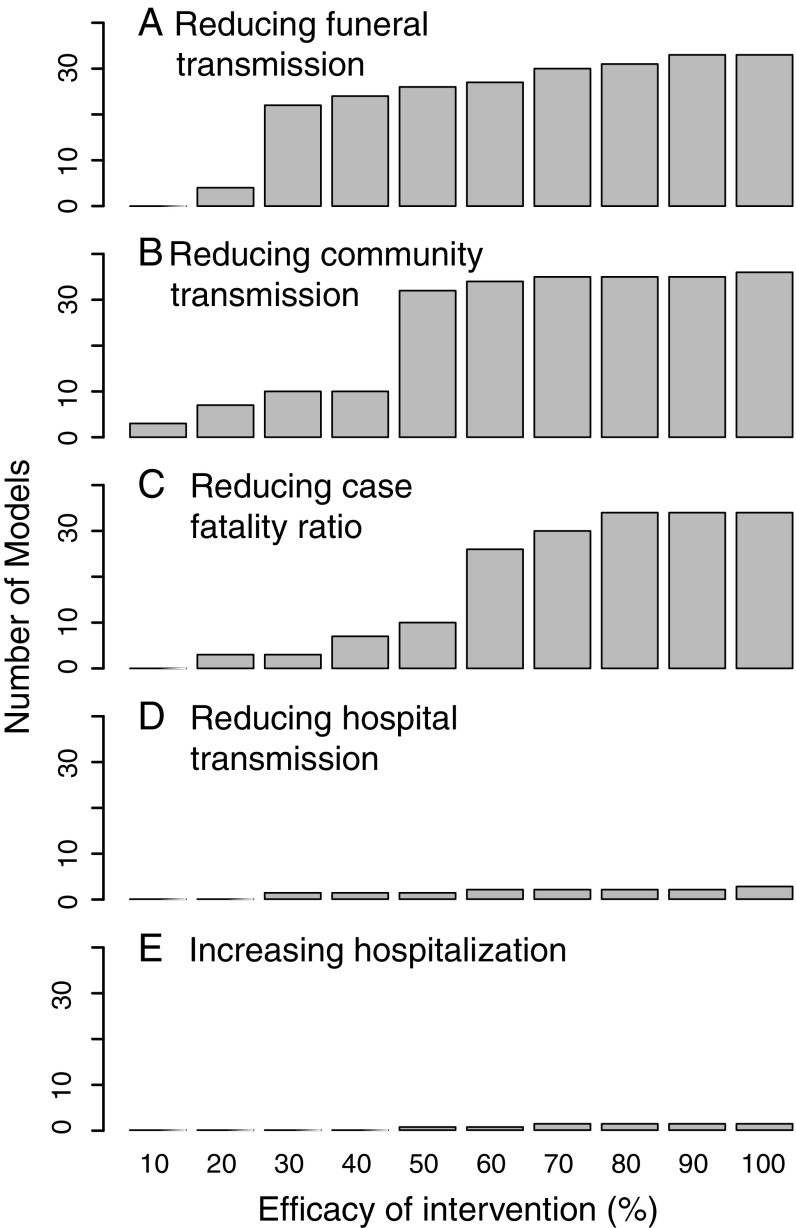
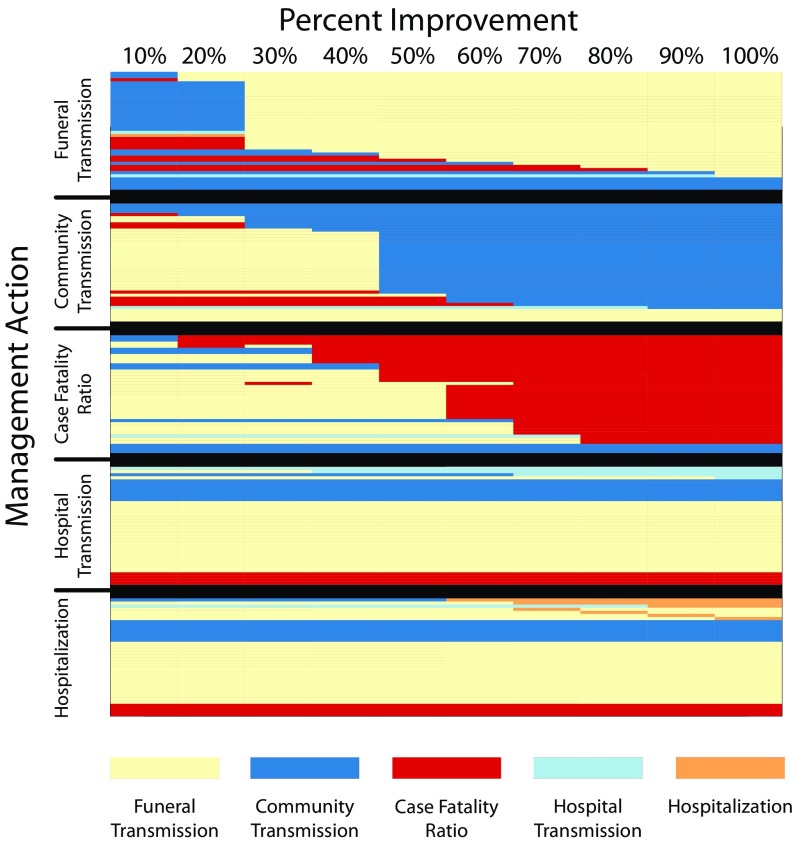
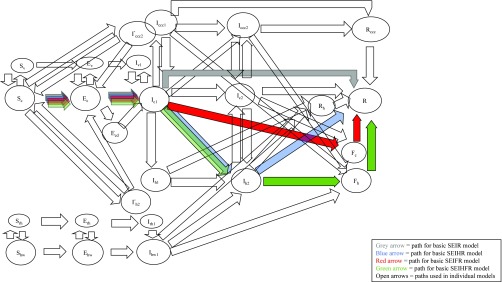
Early resolution of uncertainty during an epidemic outbreak can lead to rapid and efficient decision making, provided that the uncertainty affects prioritization of actions. The wide range in caseload projections for the 2014 Ebola outbreak caused great concern and debate about the utility of models. By coding and running 37 published Ebola models with five candidate interventions, we found that, despite this large variation in caseload projection, the ranking of management options was relatively consistent. Reducing funeral transmission and reducing community transmission were generally ranked as the two best options. Value of information (VoI) analyses show that caseloads could be reduced by 11% by resolving all model-specific uncertainties, with information about model structure accounting for 82% of this reduction and uncertainty about caseload only accounting for 12%. Our study shows that the uncertainty that is of most interest epidemiologically may not be the same as the uncertainty that is most relevant for management. If the goal is to improve management outcomes, then the focus of study should be to identify and resolve those uncertainties that most hinder the choice of an optimal intervention. Our study further shows that simplifying multiple alternative models into a smaller number of relevant groups (here, with shared structure) could streamline the decision-making process and may allow for a better integration of epidemiological modeling and decision making for policy.
Keywords: VoI; decision making; epidemiological outbreak management; value of information.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Butler D. Models overestimate Ebola cases. Nature. 2014;515:18. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
