

Subcutaneous golimumab for children with active polyarticular-course juvenile idiopathic arthritis: results of a multicentre, double-blind, randomised-withdrawal trial
- PMID: 28507219
- PMCID: PMC5754736
- DOI: 10.1136/annrheumdis-2016-210456
Subcutaneous golimumab for children with active polyarticular-course juvenile idiopathic arthritis: results of a multicentre, double-blind, randomised-withdrawal trial
Abstract
Objective: This report aims to determine the safety, pharmacokinetics (PK) and efficacy of subcutaneous golimumab in active polyarticular-course juvenile idiopathic arthritis (polyJIA).
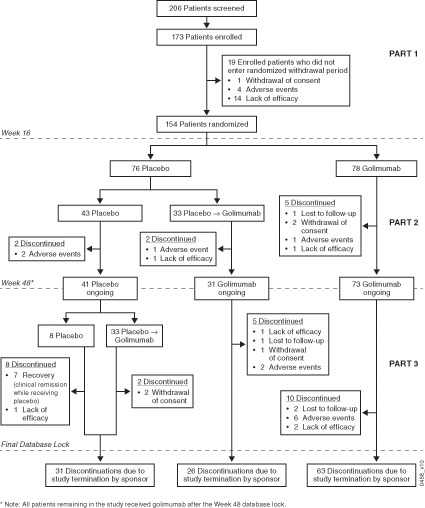
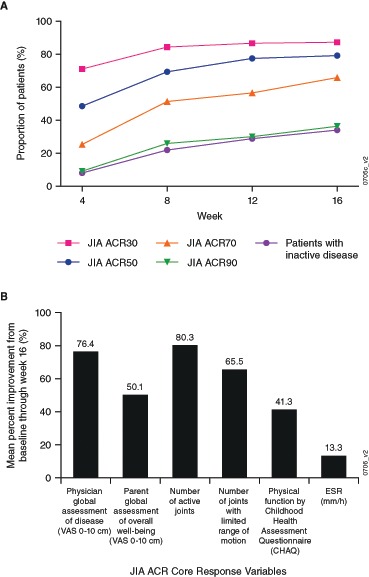
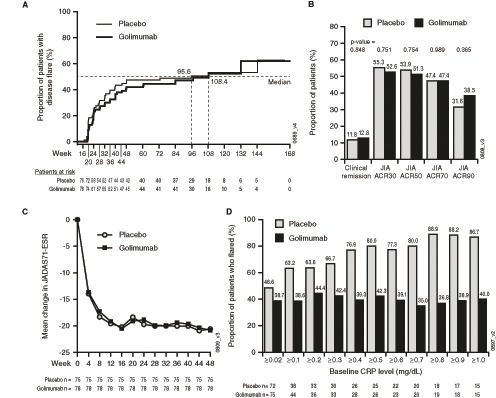
Methods: In this three-part randomised double-blinded placebo-controlled withdrawal trial, all patients received open-label golimumab (30 mg/m2 of body surface area; maximum: 50 mg/dose) every 4 weeks together with weekly methotrexate during Part 1 (weeks 0-16). Patients with at least 30% improvement per American College of Rheumatology Criteria for JIA (JIA ACR30) in Part 1 entered the double-blinded Part 2 (weeks 16-48) after 1:1 randomisation to continue golimumab or start placebo. In Part 3, golimumab was continued or could be restarted as in Part 1. The primary outcome was JIA flares in Part 2; secondary outcomes included JIA ACR50/70/90 responses, clinical remission, PK and safety.
Results: Among 173 patients with polyJIA enrolled, 89.0% (154/173) had a JIA ACR30 response and 79.2%/65.9%/36.4% demonstrated JIA ACR50/70/90 responses in Part 1. At week 48, the primary endpoint was not met as treatment groups had comparable JIA flare rates (golimumab vs placebo: 32/78=41% vs 36/76=47%; p=0.41), and rates of clinical remission were comparable (golimumab vs placebo: 10/78=12.8% vs 9/76=11.8%). Adverse event and serious adverse event rates were similar in the treatment groups during Part 2. Injection site reactions occurred with <1% of all injections. PK analysis confirmed adequate golimumab dosing for polyJIA.
Conclusion: Although the primary endpoint was not met, golimumab resulted in rapid, clinically meaningful, improvement in children with active polyJIA. Golimumab was well tolerated, and no unexpected safety events occurred.
Clinical trial registration: NCT01230827; Results.
Keywords: anti-tumour necrosis factor; biologics; golimumab; juvenile idiopathic arthritis.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: HIB has served as a consultant and steering committee member for Janssen Research & Development, a consultant for AstraZeneca, Pfizer and Takeda and received research support from Novartis, Roche and UCB. NR served on the speaker’s bureau and as a consultant for AbbVie, Amgen, Alter, AstraZeneca, Baxalta Biosimilars, Biogen Idec, Boehringer, BMS, Celgene, CrescendoBio, EMD Serono, F. Hoffmann-La Roche, Italfarmaco, Janssen, MedImmune, Medac, Novartis, Novo Nordisk, Pfizer, Sanofi Aventis, Servier, Takeda and UCB Biosciences GmbH. DJL has served as a consultant for Boehringer Ingelheim, Celgene, Janssen Research & Development and Novartis, as a trial investigator for AbbVie, Bristol-Myers Squibb, Janssen Research & Development, Roche, Pfizer and UBC and received research support from the National Institutes of Health. NRP received fees from AbbVie and Roche. FS received research support from Janssen. KM received research support from Pfizer, AbbVie, Roche and Deutsche Kinder-Rheumastiftung and fees from AbbVie, Genzyme, Medac, Pfizer and Pharm-Allergan. IN received fees from AbbVie, Bristol-Myers Squibb, Novartis, Pfizer and Roche and grants from Pfizer and Roche. EA received research support from AbbVie, Bristol-Myers Squibb, Janssen, Novartis, Pfizer and Roche and fees from AbbVie, Bristol-Myers Squibb, Medac, Merck Sharp & Dohme, Novartis, Pfizer and Roche. KEG, ZX, JHL, LK, SLL and MJL are employees of Janssen Research & Development, LLC and own stock in Johnson & Johnson. AM received speaking and consulting fees from AbbVie, Boehringer, Celgene, CrescendoBio, Janssen, MedImmune, Novartis, Novo Nordisk, Pfizer, Sanofi Aventis, Vertex and Servier. Nothing to disclose: NT, GH, VGC, CAM, AR, DJK, EDS, VP, MRMV, ES, MB, ARK, VK, RJ, WE, IF, BRL.
Figures
Comment in
-
Learning the hard way: clinical trials in juvenile idiopathic arthritis.Ann Rheum Dis. 2018 Jan;77(1):1-2. doi: 10.1136/annrheumdis-2017-211108. Epub 2017 May 25. Ann Rheum Dis. 2018. PMID: 28546255 No abstract available.
References
-
- Petty RE, Southwood TR, Manners P, et al. ; International League of Associations for Rheumatology. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol 2004;31:390–2. - PubMed
-
- Beukelman T, Patkar NM, Saag KG, et al. 2011 American College of Rheumatology recommendations for the treatment of juvenile idiopathic arthritis: initiation and safety monitoring of therapeutic agents for the treatment of arthritis and systemic features. Arthritis Care Res 2011;63:465–82. 10.1002/acr.20460 - DOI - PMC - PubMed
-
- Simponi: package insert. Janssen Biotech, Inc: Horsham, PA, 2014.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
