

Randomized, Multicenter Trial of ARTSS-2 (Argatroban With Recombinant Tissue Plasminogen Activator for Acute Stroke)
- PMID: 28507269
- PMCID: PMC5499711
- DOI: 10.1161/STROKEAHA.117.016720
Randomized, Multicenter Trial of ARTSS-2 (Argatroban With Recombinant Tissue Plasminogen Activator for Acute Stroke)
Abstract
Background and purpose: We conducted a randomized exploratory study to assess safety and the probability of a favorable outcome with adjunctive argatroban, a direct thrombin-inhibitor, administered to recombinant tissue-type plasminogen activator (r-tPA)-treated ischemic stroke patients.
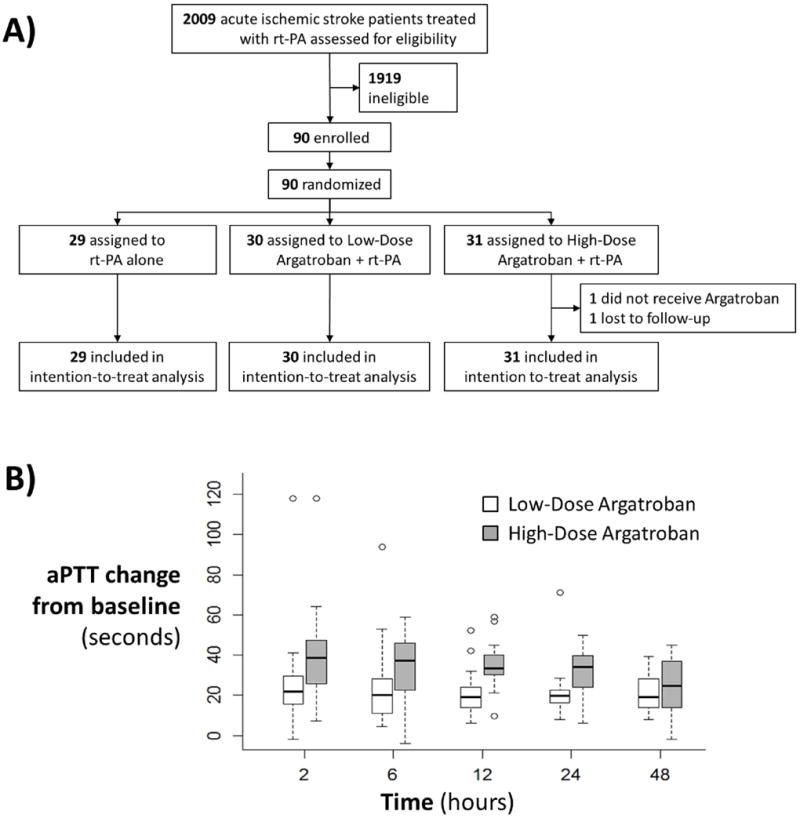
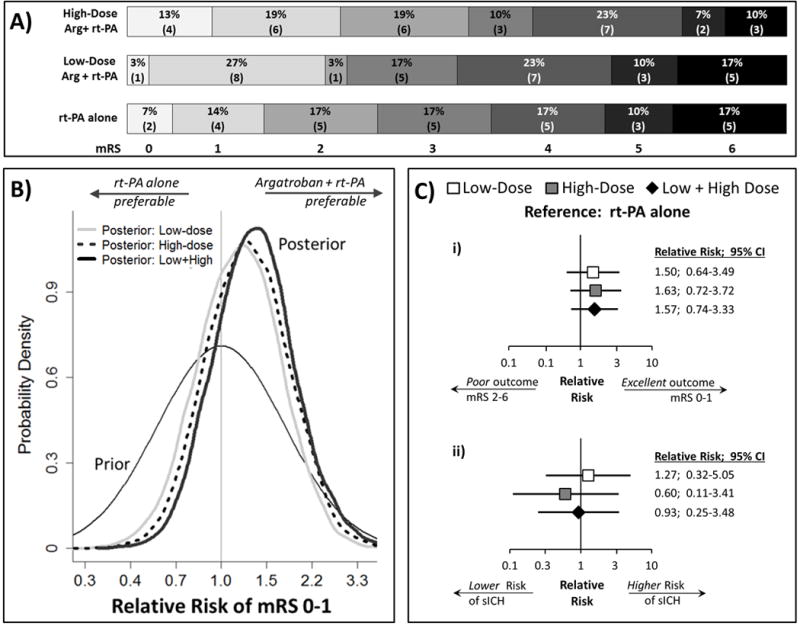
Methods: Patients treated with standard-dose r-tPA, not receiving endovascular therapy, were randomized to receive no argatroban or argatroban (100 μg/kg bolus) followed by infusion of either 1 (low dose) or 3 μg/kg per minute (high dose) for 48 hours. Safety was incidence of symptomatic intracerebral hemorrhage. Probability of clinical benefit (modified Rankin Scale score 0-1 at 90 days) was estimated using a conservative Bayesian Poisson model (neutral prior probability centered at relative risk, 1.0 and 95% prior intervals, 0.33-3.0).
Results: Ninety patients were randomized: 29 to r-tPA alone, 30 to r-tPA+low-dose argatroban, and 31 to r-tPA+high-dose argatroban. Rates of symptomatic intracerebral hemorrhage were similar among control, low-dose, and high-dose arms: 3/29 (10%), 4/30 (13%), and 2/31 (7%), respectively. At 90 days, 6 (21%) r-tPA alone, 9 (30%) low-dose, and 10 (32%) high-dose patients were with modified Rankin Scale score 0 to 1. The relative risks (95% credible interval) for modified Rankin Scale score 0 to 1 with low, high, and either low or high dose argatroban were 1.17 (0.57-2.37), 1.27 (0.63-2.53), and 1.34 (0.68-2.76), respectively. The probability that adjunctive argatroban was superior to r-tPA alone was 67%, 74%, and 79% for low, high, and low or high dose, respectively.
Conclusions: In patients treated with r-tPA, adjunctive argatroban was not associated with increased risk of symptomatic intracerebral hemorrhage and provides evidence that a definitive effectiveness trial is indicated.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique Identifier: NCT01464788.
Keywords: acute stroke; adjunctive therapy; anticoagulation; argatroban; randomized controlled trial; thrombin inhibitor; thrombolysis.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Response by Barreto and Grotta to Letter Regarding Article, "Randomized, Multicenter Trial of ARTSS-2 (Argatroban With Recombinant Tissue Plasminogen Activator for Acute Stroke)".Stroke. 2017 Sep;48(9):e259. doi: 10.1161/STROKEAHA.117.018294. Epub 2017 Jul 28. Stroke. 2017. PMID: 28754829 Free PMC article. No abstract available.
-
Letter by Shah Regarding Article, "Randomized, Multicenter Trial of ARTSS-2 (Argatroban With Recombinant Tissue Plasminogen Activator for Acute Stroke)".Stroke. 2017 Sep;48(9):e258. doi: 10.1161/STROKEAHA.117.018121. Epub 2017 Jul 28. Stroke. 2017. PMID: 28754831 No abstract available.
References
-
- Alexandrov AV, Grotta JC. Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator. Neurology. 2002;59:862–867. - PubMed
-
- Saqqur M, Uchino K, Demchuk AM, Molina CA, Garami Z, Calleja S, et al. Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke. Stroke. 2007;38:948–954. - PubMed
-
- Tamao Y, Kikumoto R. Effect of argatroban, a selective thrombin inhibitor, on animal models of cerebral thrombosis. Semin Thromb Hemost. 1997;23:523–530. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
