

Fingolimod initiation in multiple sclerosis patients is associated with potential beneficial cardiovascular autonomic effects
- PMID: 28507603
- PMCID: PMC5415227
- DOI: 10.1177/1756285616682936
Fingolimod initiation in multiple sclerosis patients is associated with potential beneficial cardiovascular autonomic effects
Abstract
Background: Fingolimod slows heart rate (HR) due to vagomimetic effects and might cause additional cardiovascular autonomic changes. While the time course of HR changes is well described, the extent and course of cardiovascular autonomic changes upon fingolimod initiation has not yet been evaluated. This study, therefore, intended to assess cardiovascular autonomic changes during the first 6 h after fingolimod initiation.
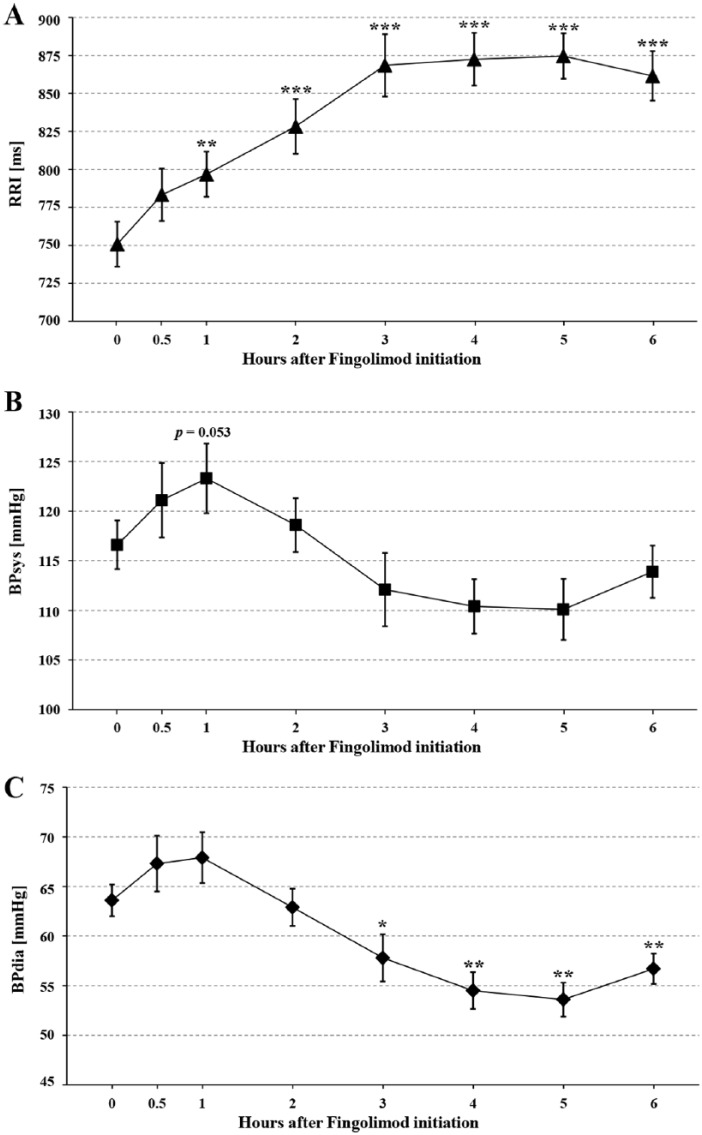
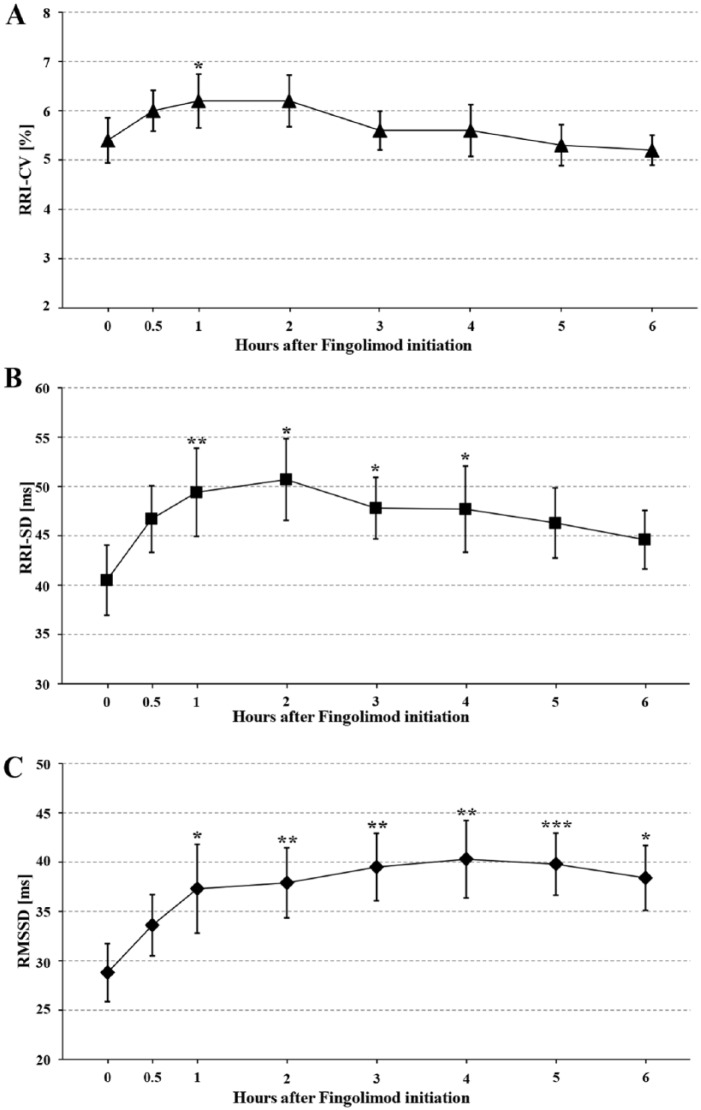
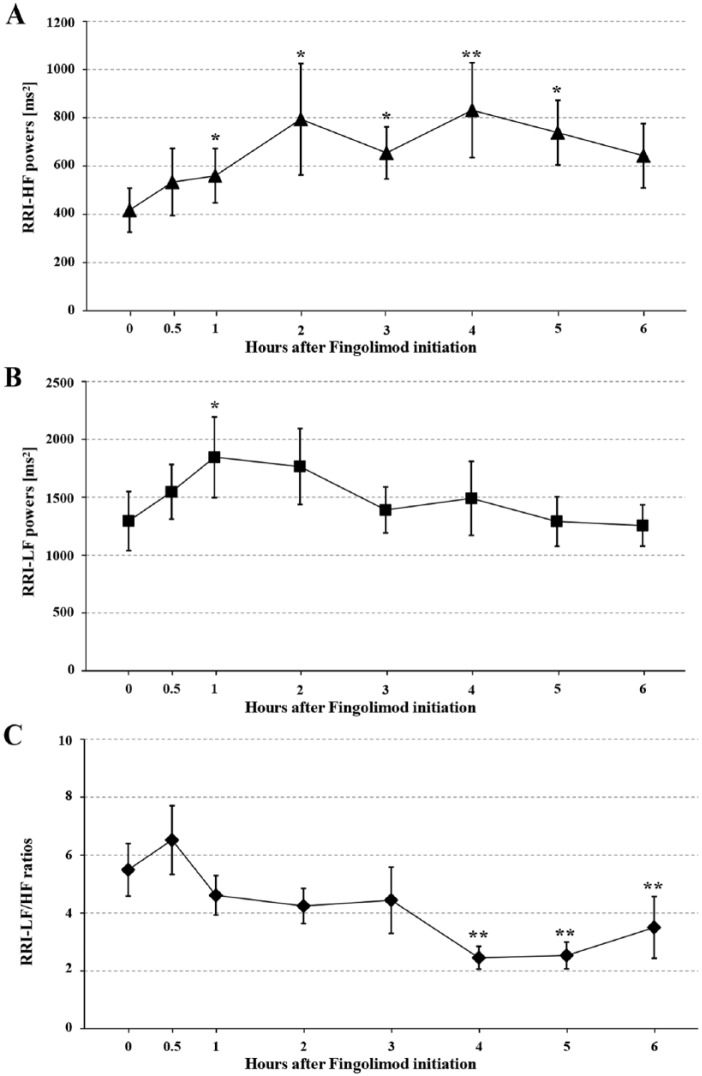
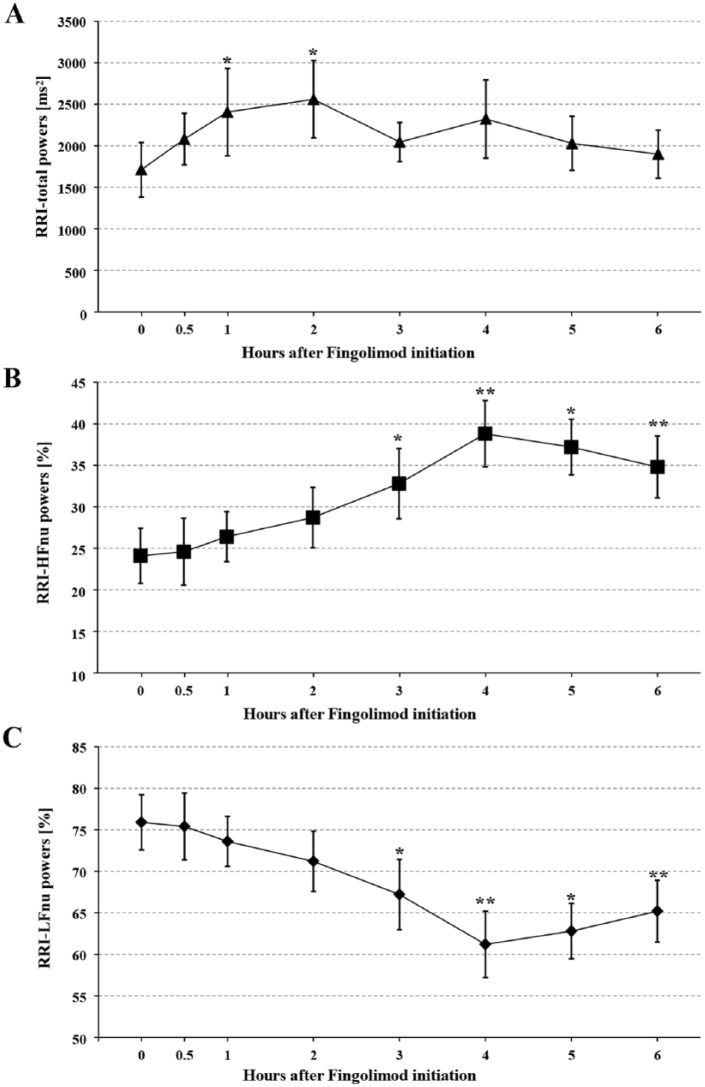
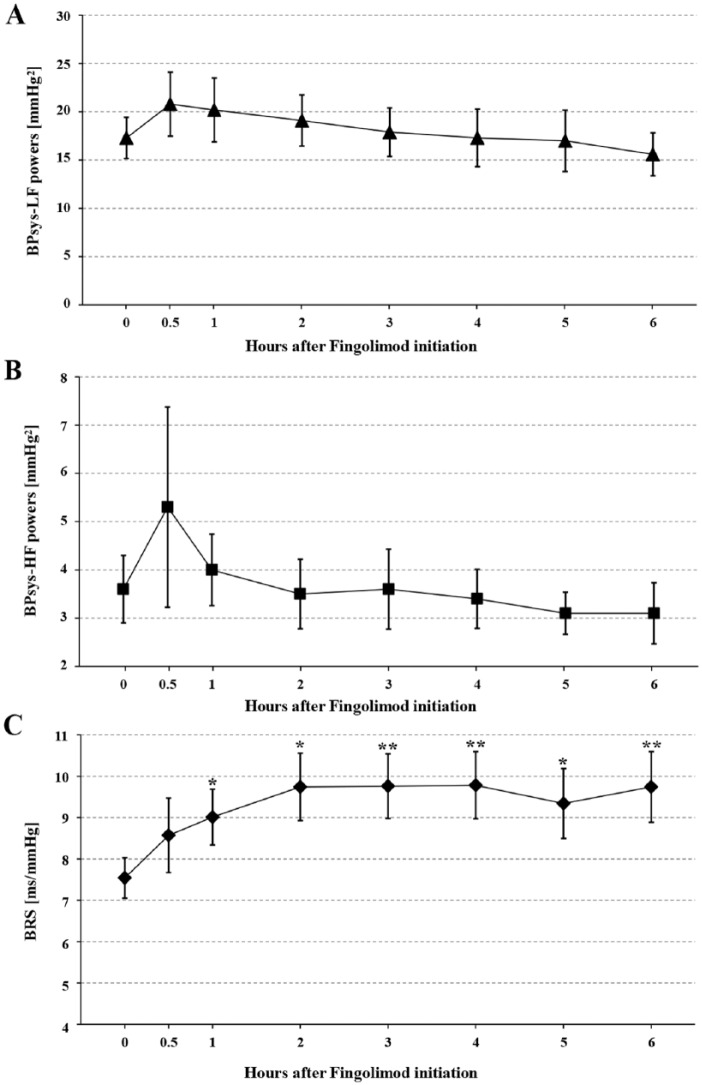
Methods: In 21 patients with relapsing-remitting multiple sclerosis (RRMS), we recorded respiration (RESP), electrocardiographic RR interval (RRI), systolic and diastolic blood pressure (BPsys, BPdia) at rest, before and 0.5, 1, 2, 3, 4, 5, and 6 h after fingolimod initiation. We calculated parameters of total autonomic modulation [RRI standard deviation (RRI-SD), RRI coefficient of variation (RRI-CV), RRI-total powers], mainly sympathetic cardiac modulation [RRI low frequency (LF) powers], sympathetic BP modulation (BPsys-LF powers), parasympathetic modulation [square root of the mean squared difference of successive RRIs (RMSSD), RRI high frequency (HF) powers], sympatho-vagal cardiac balance (RRI-LF/HF ratios), and baroreflex sensitivity (BRS). We compared parameters between the eight measurements [analysis of variance (ANOVA) or Friedman test with post-hoc analysis; significance: p < 0.05].
Results: After fingolimod initiation, RESP, BPsys, and BPsys-LF powers remained unchanged while RRIs, RRI-CV, RRI-SD, RRI-total powers, RRI-LF powers, RMSSD, RRI-HF powers, and BRS increased after 1 h and rose to peak values occurring after 5, 1, 2, 2, 1, 4, 4, and 4 h, respectively. After 3 h, BPdia had decreased significantly and was lowest after 5 h. RRI-LF/HF ratios decreased to a nadir after 4 h.
Conclusions: The increases in parasympathetic and overall cardiac autonomic modulation and in BRS seen with fingolimod initiation are theoretically beneficial for the MS patient's cardiovascular system. However, long-term studies must show whether these effects persist or are attenuated (e.g. due to S1P1 receptor down-regulation upon continued fingolimod therapy).
Keywords: cardiovascular autonomic modulation; fingolimod; multiple sclerosis.
Conflict of interest statement
Conflict of interest statement: The authors declared the following potential conflicts of interest with respect to the research, authorship, or publication of this article: MJH has received personal compensation for activities from Genzyme, A Sanofi Company (Germany). MJH has received research support from the Rolf and Hubertine Schiffbauer Foundation, Bayer Health Care (Germany) and Novartis Pharma GmbH, Germany. CRL has received travel grants from Genzyme, A Sanofi Company. FC has received travel grants from Genzyme, A Sanofi Company. DHL has received travel grants or speaker honoraria from Bayer Health Care Pharmaceuticals (NJ, USA), Biogen Idec (Cambridge, MA, USA), Merck Serono (Germany), Novartis Pharma GmbH, and TEVA Pharmaceutical Industries (Germany). RAL has received travel grants or speaker honoraria from Bayer Health Care Pharmaceuticals, Biogen Idec, Merck Serono, Novartis Pharma GmbH, Roche (Switzerland), and TEVA Pharmaceutical Industries Ltd. RAL has received research support from Novartis Pharma GmbH, Biogen Idec, and Merck Serono. RW, ML, SR, KHM and KW declare that there is no conflict of interest.
Figures
Similar articles
-
S1P receptor modulators and the cardiovascular autonomic nervous system in multiple sclerosis: a narrative review.Ther Adv Neurol Disord. 2022 Nov 22;15:17562864221133163. doi: 10.1177/17562864221133163. eCollection 2022. Ther Adv Neurol Disord. 2022. PMID: 36437849 Free PMC article. Review.
-
Pre-existing parasympathetic dominance seems to cause persistent heart rate slowing after 6 months of fingolimod treatment in patients with multiple sclerosis.Clin Auton Res. 2025 Feb;35(1):59-73. doi: 10.1007/s10286-024-01073-w. Epub 2024 Oct 9. Clin Auton Res. 2025. PMID: 39382757 Free PMC article.
-
Cardiovascular autonomic regulation correlates with cognitive performance in patients with a history of traumatic brain injury.Neurol Sci. 2023 Oct;44(10):3535-3544. doi: 10.1007/s10072-023-06857-y. Epub 2023 May 25. Neurol Sci. 2023. PMID: 37227563 Free PMC article.
-
Valsalva maneuver unveils central baroreflex dysfunction with altered blood pressure control in persons with a history of mild traumatic brain injury.BMC Neurol. 2016 May 4;16:61. doi: 10.1186/s12883-016-0584-5. BMC Neurol. 2016. PMID: 27146718 Free PMC article.
-
Heart rate variability and autonomic activity at rest and during exercise in various physiological conditions.Eur J Appl Physiol. 2003 Oct;90(3-4):317-25. doi: 10.1007/s00421-003-0953-9. Epub 2003 Sep 12. Eur J Appl Physiol. 2003. PMID: 13680241 Review.
Cited by
-
Modulation of Cardiac Autonomic Function by Fingolimod Initiation and Predictors for Fingolimod Induced Bradycardia in Patients with Multiple Sclerosis.Front Neurosci. 2017 Oct 12;11:540. doi: 10.3389/fnins.2017.00540. eCollection 2017. Front Neurosci. 2017. PMID: 29075174 Free PMC article.
-
Cardiovascular fingolimod effects on rapid baroreceptor unloading are counterbalanced by baroreflex resetting.Neurol Sci. 2021 Jan;42(1):111-121. doi: 10.1007/s10072-020-05004-1. Epub 2021 Jan 14. Neurol Sci. 2021. PMID: 33443674 Free PMC article.
-
Long-term effects of siponimod on cardiovascular and autonomic nervous system in secondary progressive multiple sclerosis.Front Pharmacol. 2024 Sep 19;15:1431380. doi: 10.3389/fphar.2024.1431380. eCollection 2024. Front Pharmacol. 2024. PMID: 39364051 Free PMC article.
-
S1P receptor modulators and the cardiovascular autonomic nervous system in multiple sclerosis: a narrative review.Ther Adv Neurol Disord. 2022 Nov 22;15:17562864221133163. doi: 10.1177/17562864221133163. eCollection 2022. Ther Adv Neurol Disord. 2022. PMID: 36437849 Free PMC article. Review.
-
Cardiac Autonomic Dysfunction in Multiple Sclerosis: A Systematic Review of Current Knowledge and Impact of Immunotherapies.J Clin Med. 2020 Jan 24;9(2):335. doi: 10.3390/jcm9020335. J Clin Med. 2020. PMID: 31991711 Free PMC article. Review.
References
-
- Abdullah C., Li Z., Wang X., Jin Z. (2016) Depletion of T lymphocytes ameliorates cardiac fibrosis in streptozotocin-induced diabetic cardiomyopathy. Int Immunopharmacol 39: 251–264. - PubMed
-
- Brown C., Hecht M., Weih A., Neundorfer B., Hilz M. (2003) Effects of age on the cardiac and vascular limbs of the arterial baroreflex. Eur J Clin Invest 33: 10–16. - PubMed
-
- Camm J., Hla T., Bakshi R., Brinkmann V. (2014) Cardiac and vascular effects of fingolimod: mechanistic basis and clinical implications. Am Heart J 168: 632–644. - PubMed
-
- Cohen J., Barkhof F., Comi G., Hartung H., Khatri B., Montalban X., et al. (2010) Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med 362: 402–415. - PubMed
-
- Cutter G., Baier M., Rudick R., Cookfair D., Fischer J., Petkau J., et al. (1999) Development of a multiple sclerosis functional composite as a clinical trial outcome measure. Brain 122: 871–882. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
