

Spinal osteotomies: indications, limits and pitfalls
- PMID: 28507779
- PMCID: PMC5420824
- DOI: 10.1302/2058-5241.2.160069
Spinal osteotomies: indications, limits and pitfalls
Abstract
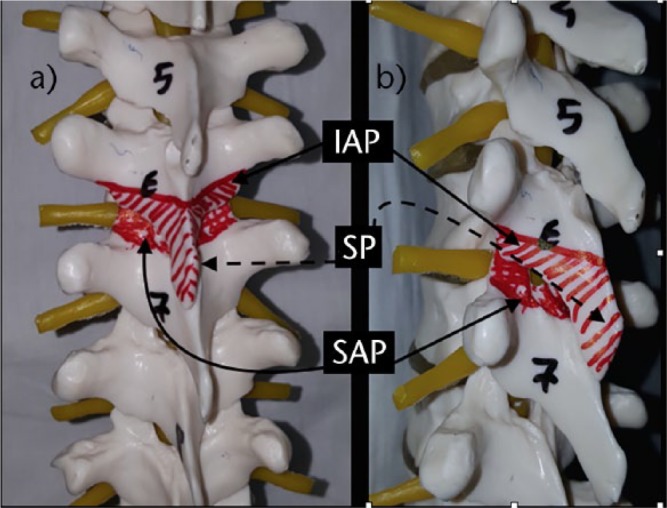
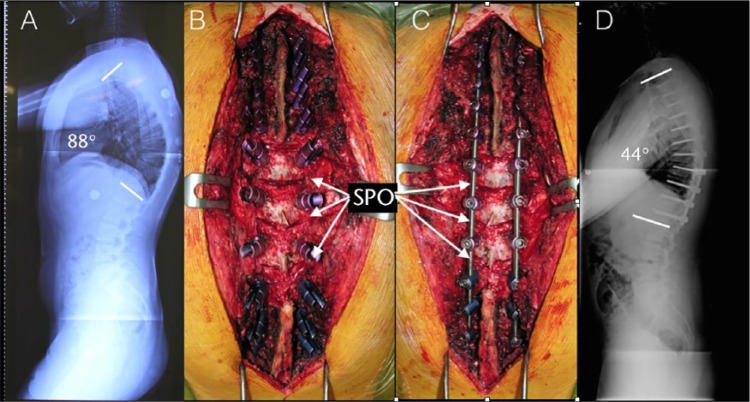
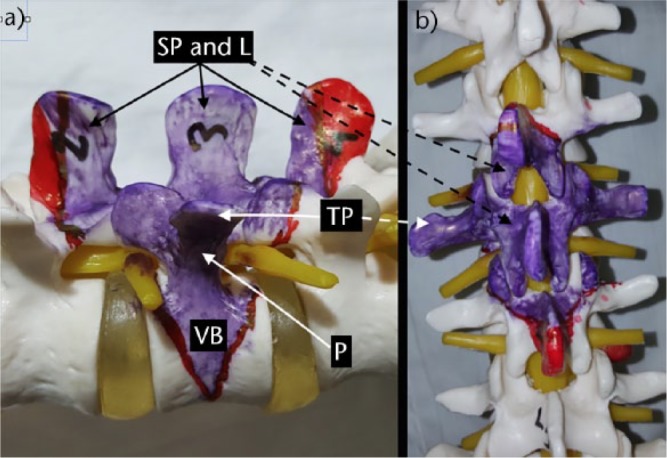
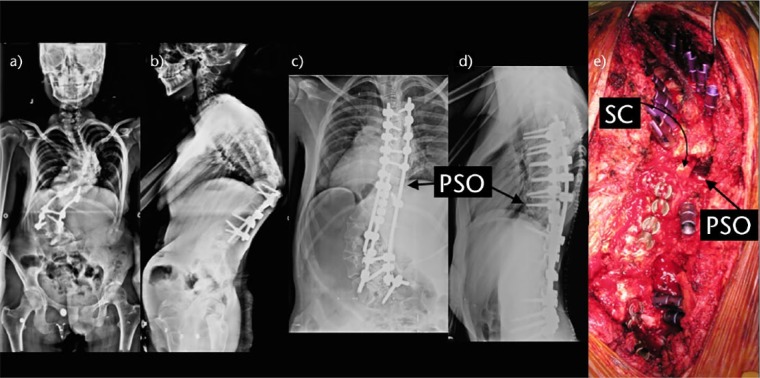
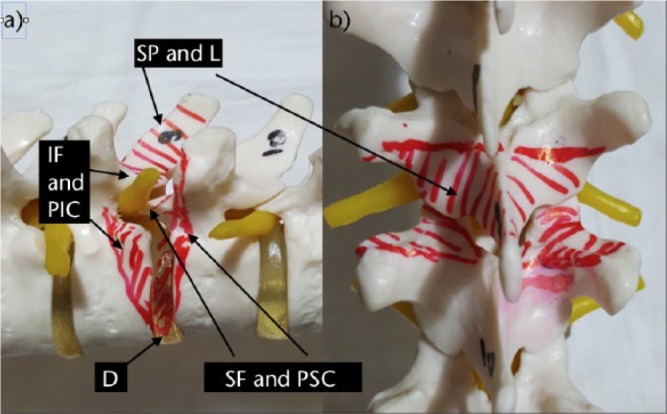
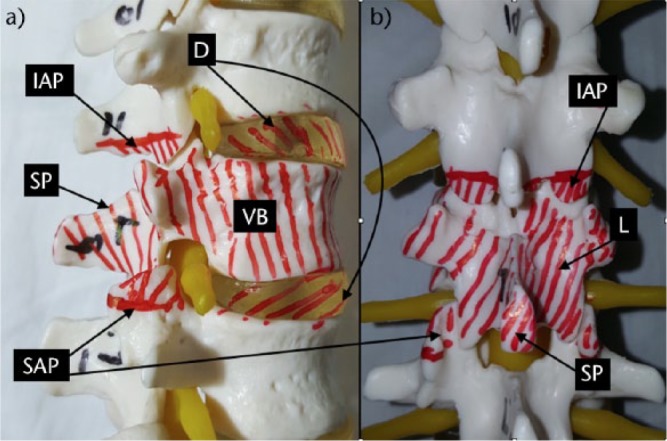
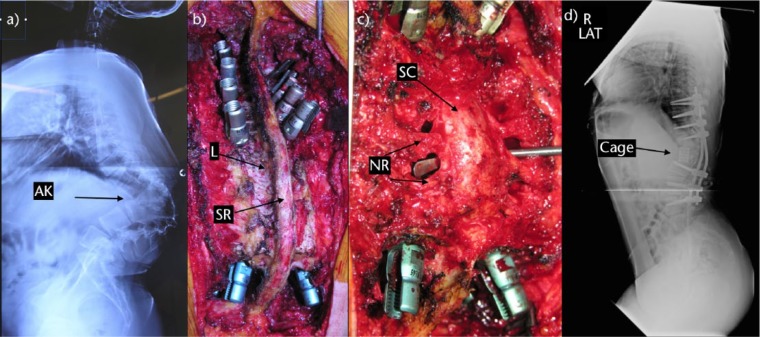
The aims of spinal deformity surgery are to achieve balance, relieve pain and prevent recurrence or worsening of the deformity.The main types of osteotomies are the Smith-Petersen osteotomy (SPO), pedicle subtraction osteotomy (PSO), bone-disc-bone osteotomy (BDBO) and vertebral column resection (VCR), in order of increasing complexity.SPO is a posterior column osteotomy in which the posterior ligaments and the facet joints are removed and correction is performed through the disc space. A mobile anterior disc is essential. SPO is best in patients with +6-8 cm C7 plumbline. The amount of correction is 9.3° to 10.7°/level (1°/mm bone).PSO is a technique where the posterior elements and pedicles are removed. Then a triangular wedge through the pedicles is removed and the posterior spine is shortened using the anterior cortex as a hinge. The ideal candidates are patients with a severe sagittal imbalance. A single level osteotomy can produce 30° 40° of correction. A single level osteotomy may restore global sagittal balance by an average of 9 cm with an upper limit of 19 cm.BDBO is an osteotomy done above and below a disc level. A BDBO provides correction rates in the range of 35° to 60°. The main indications are deformities with the disc space as the apex and severe sagittal plane deformities.VCR is indicated for rigid multi-planar deformities, sharp angulated deformities, hemivertebra resections, resectable spinal tumours, post-traumatic deformities and spondyloptosis. The main indication for a VCR is fixed coronal plane deformity.The type of osteotomy must be chosen mainly according to the aetiology, type and apex of the deformity. One may start with SPOs and may gradually advance to complex osteotomies. Cite this article: EFORT Open Rev 2017;2:73-82. DOI: 10.1302/2058-5241.2.160069.
Conflict of interest statement
ICMJE Conflict of Interest Statement: None
Figures

References
-
- Smith-Petersen MN, Larson EB, AuFranc OE. Osteotomy of the spine for correction of flexion deformity in rheumatoid arthritis. J Bone Joint Surg [Am] 1945;27-A:1-11. - PubMed
-
- Ponte A, Vero B, Siccardi GL. Surgical treatment of Scheuermann’s kyphosis. In: Winter RB, ed. Progress in spinal pathology: kyphosis. Bologna: Aulo Gaggi, 1984:75-80.
-
- Bridwell KH. Decision making regarding Smith-Petersen vs. pedicle subtraction osteotomy vs. vertebral column resection for spinal deformity. Spine (Phila Pa 1976) 2006;31:S171-S178. - PubMed
-
- Dorward IG, Lenke LG. Osteotomies in the posterior-only treatment of complex adult spinal deformity: a comparative review. Neurosurg Focus 2010;28:E4. - PubMed
-
- Lafage V, Schwab F, Patel A, Hawkinson N, Farcy JP. Pelvic tilt and truncal inclination: two key radiographic parameters in the setting of adults with spinal deformity. Spine (Phila Pa 1976) 2009;34:E599-E606. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
