

Spine Stereotactic Body Radiotherapy: Indications, Outcomes, and Points of Caution
- PMID: 28507888
- PMCID: PMC5415159
- DOI: 10.1177/2192568217694016
Spine Stereotactic Body Radiotherapy: Indications, Outcomes, and Points of Caution
Abstract
Study design: A broad narrative review.
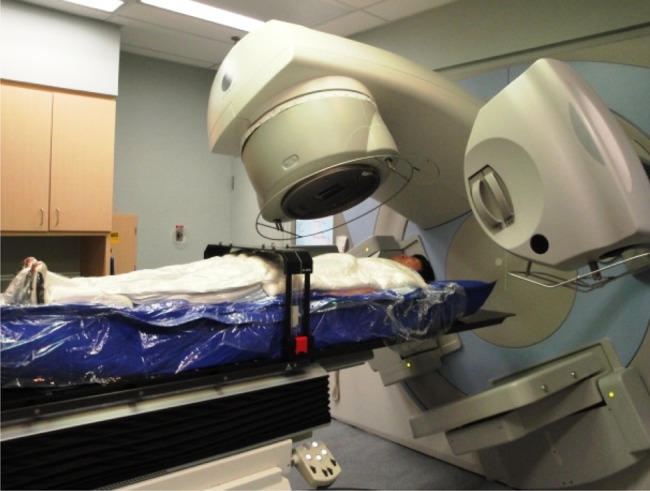
Objectives: The objective of this article is to provide a technical review of spine stereotactic body radiotherapy (SBRT) planning and delivery, indications for treatment, outcomes, complications, and the challenges of response assessment. The surgical approach to spinal metastases is discussed with an overview of emerging minimally invasive techniques.
Methods: A comprehensive review of the literature was conducted on the techniques, outcomes, and developments in SBRT and surgery for spinal metastases.
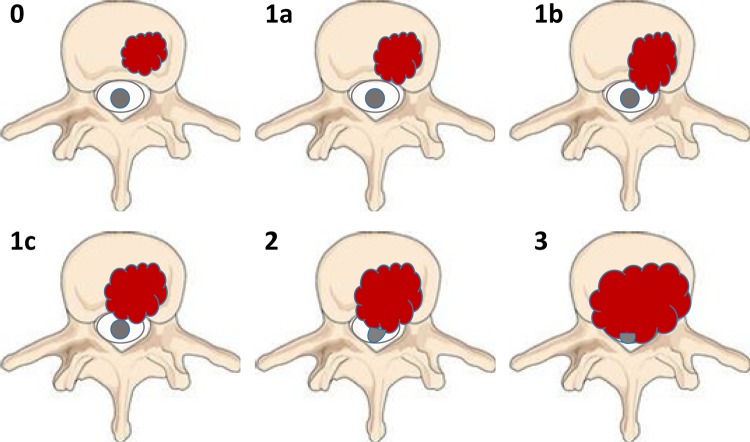
Results: The optimal management of patients with spinal metastases is complex and requires multidisciplinary assessment from an oncologic team that is familiar with the shifting paradigm as a consequence of evolving techniques in surgery and stereotactic radiation, as well as new developments in systemic agents. The Spinal Instability Neoplastic Score and the epidural spinal cord compression (Bilsky) grading system are useful tools that facilitate communication among oncologic team members and can direct management by providing a baseline assessment of risks prior to therapy. The combined multimodality approach with "separation surgery" followed by postoperative spine SBRT achieves thecal sac decompression, improves tumor control, and avoids complications that may be associated with more extensive surgery.
Conclusion: Spine SBRT is a highly effective treatment that is capable of delivering ablative doses to the target while sparing the critical organs-at-risk, chiefly the critical neural tissues, within a short and manageable schedule. At the same time, surgery occupies an important role in select patients, particularly with the expanding availability and expertise in minimally invasive techniques. With rapid adoption of spine SBRT in centers outside of the academic setting, it is imperative for the practicing oncologist to understand the relevance and application of these evolving concepts.
Keywords: postoperative radiation; spinal cord compression; spine metastasis; spine radiosurgery; spine stereotactic body radiotherapy.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Arjun Sahgal has received honorarium for previous educational seminars from Medtronic Kyphoplasty Division and Elekta AB, research grants from Elekta AB. Dr Hany Soliman has received travel support from Elekta AB for research conferences. Dr Simon Lo has received research support through International Oligometastasis Consortium from Elekta AB, and travel expenses and honorarium for speaking in a users’ meeting from Accuray. There are no other conflicts of interest to disclose.
Figures
References
-
- Cole JS, Patchell RA. Metastatic epidural spinal cord compression. Lancet Neurol. 2008;7:459–466. doi:10.1016/S1474-4422(08)70089-9. - PubMed
-
- Galasko CS. Skeletal metastases. Clin Orthop Relat Res. 1986;(210):18–30. - PubMed
-
- De Angelis R, Sant M, Coleman MP, et al. Cancer survival in Europe 1999-2007 by country and age: results of EUROCARE–5-a population-based study. Lancet Oncol. 2014;15:23–34. doi:10.1016/S1470-2045(13)70546-1. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
