

Pauci-immune crescentic glomerulonephritis associated with use of trimethoprim-sulfamethoxazole
- PMID: 28508974
- PMCID: PMC5411645
- DOI: 10.1007/s13730-016-0222-5
Pauci-immune crescentic glomerulonephritis associated with use of trimethoprim-sulfamethoxazole
Abstract
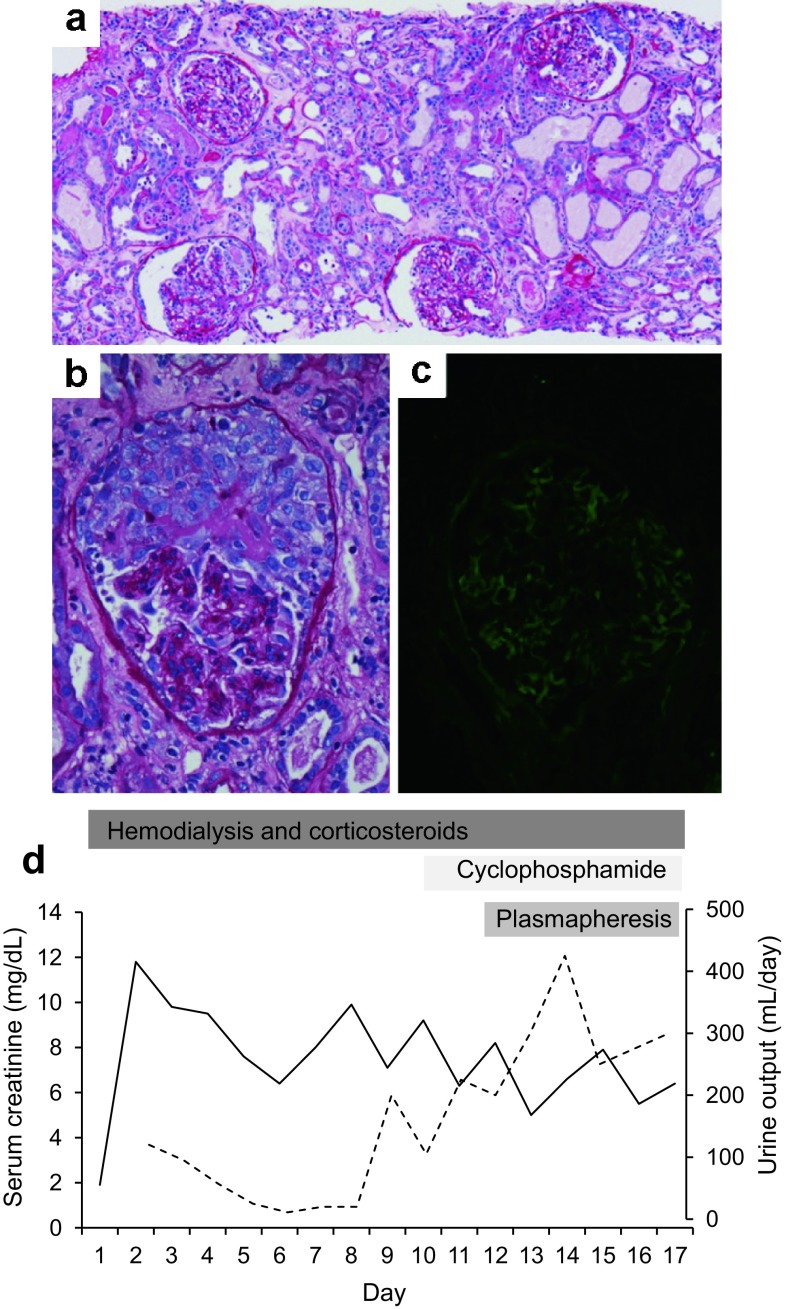
Drug-induced pauci-immune crescentic glomerulonephritis has been described with several agents, including propylthiouracil, minocycline, D-penicillamine, and hydralazine. We present the case of a 60-year-old man who presented with rapidly progressive glomerulonephritis in the setting of recent use of trimethoprim-sulfamethoxazole complicated by the development of the Stevens-Johnson syndrome, and was found to have biopsy-proven pauci-immune crescentic glomerulonephritis and undetectable anti-neutrophilic cytoplasmic antibodies. We review the existing literature on the potential association between sulfonamides and hypersensitivity polyangiitis.
Keywords: Pauci-immune crescentic glomerulonephritis; Rapidly progressive glomerulonephritis; Trimethoprim–sulfamethoxazole.
Conflict of interest statement
All the authors have declared no competing interest.
Figures
References
-
- Couser WG. Rapidly progressive glomerulonephritis: classification, pathogenic mechanisms, and therapy. Am J Kidney Dis. 1998;6:449–464. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
