

True identity of endocapillary proliferation: a case of intravascular large B cell lymphoma diagnosed with immunohistochemical study of kidney biopsy and literature review
- PMID: 28509062
- PMCID: PMC5411524
- DOI: 10.1007/s13730-012-0014-5
True identity of endocapillary proliferation: a case of intravascular large B cell lymphoma diagnosed with immunohistochemical study of kidney biopsy and literature review
Abstract
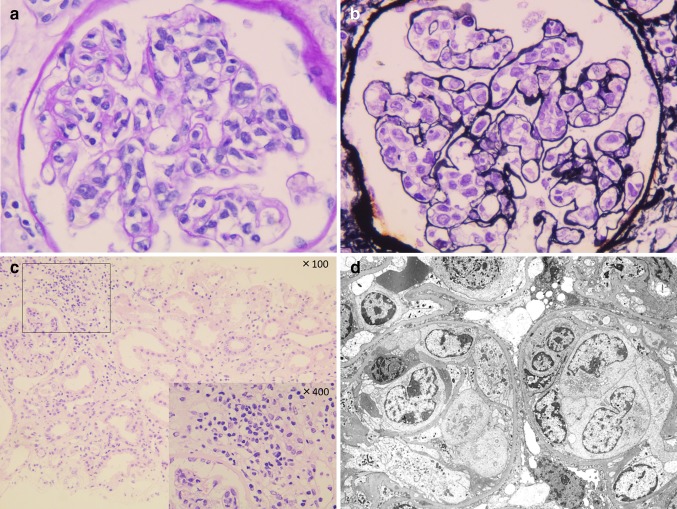
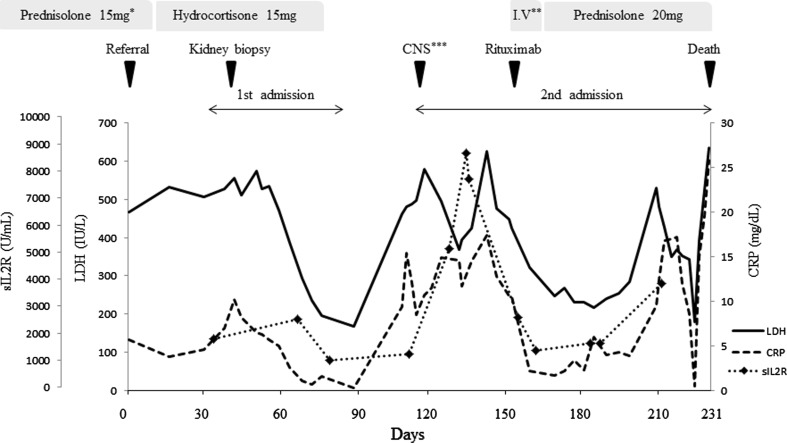
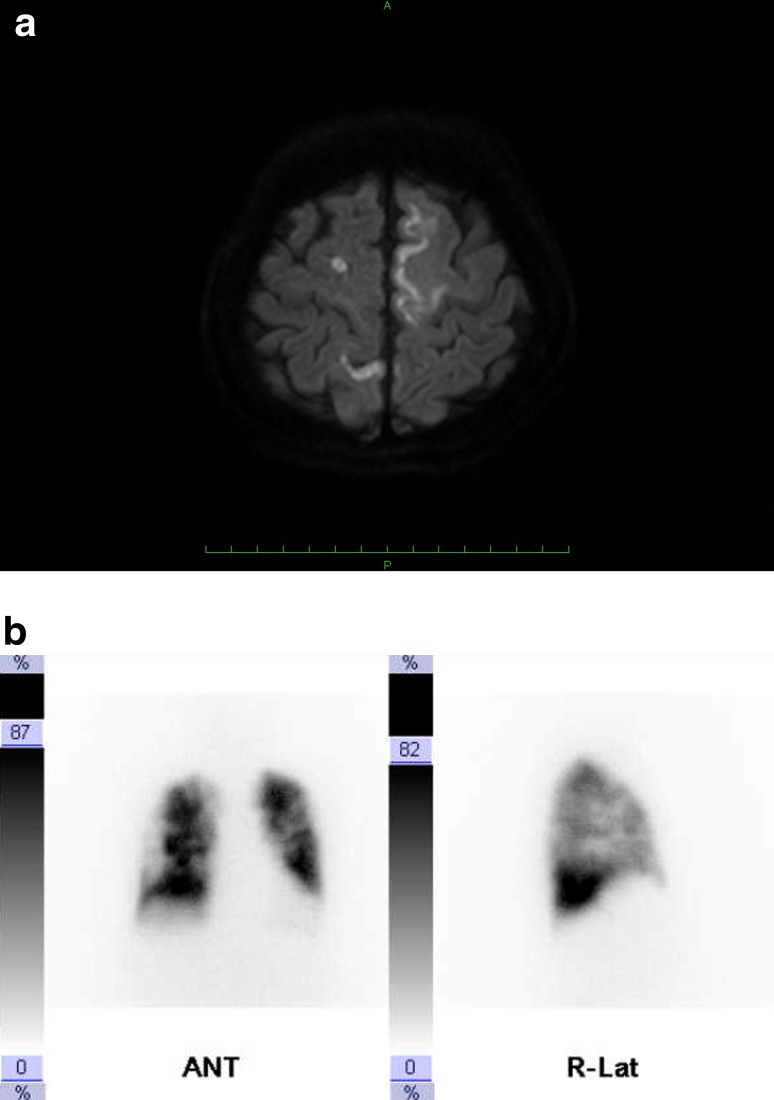
A 78-year-old Japanese female presented with low-grade fever, malaise, and appetite loss lasting for 1 month. Upper and lower gastrointestinal endoscopy and contrast-enhanced whole-body computed tomography (CT) revealed no abnormal findings at a referring hospital. She was referred to our hospital because of bilateral leg edema and 2.5 g/day proteinuria. Serum creatinine was 0.73 mg/dl and the kidneys were not enlarged. Kidney biopsy showed marked endocapillary proliferation with mesangiolysis. Soon after the kidney biopsy, her symptoms improved spontaneously, along with decreases in lactate dehydrogenase (LDH) from 503 to 197 IU/l, C-reactive protein (CRP) from 4.47 to 0.66 mg/dl, and soluble interleukin-2 receptor (sIL-2R) from 1789 to 1001 U/ml. Thus, she was followed carefully as an outpatient. One month later, however, she presented with dysarthria and right-sided hemiparesis, and diffusion-weighted brain magnetic resonance imaging (MRI) showed multiple high-intensity areas. She also had respiratory failure, and lung perfusion scintigraphy showed multiple low blood stream areas. Suspecting some endovascular abnormality, we performed immunohistochemical staining of the kidney biopsy specimen taken previously to find that endocapillary infiltrating cells were CD20-positive B lymphocytes. The infiltrating cells were confined to the endocapillary compartment in glomeruli and peritubular capillaries. Both clinical and pathological findings led us to diagnose intravascular large B cell lymphoma (IVLBCL). Two bone marrow biopsies and random skin biopsies were performed, but no abnormality was found. The present case demonstrates that clinical course and renal biopsy findings of intravascular large B cell lymphoma may mimic other renal conditions and that the identification of cell types with immunohistochemical staining may help establish an accurate diagnosis.
Keywords: Brain magnetic resonance imaging; Endocapillary proliferative glomerulonephritis; Immunohistochemical staining; Intravascular large B cell lymphoma; Kidney biopsy; Lung perfusion scintigraphy.
Figures

References
-
- Ferreri AJ, Campo E, Seymour JF, Willemze R, Ilariucci F, Ambrosetti A, et al. Intravascular lymphoma: clinical presentation, natural history, management and prognostic factors in a series of 38 cases, with special emphasis on the ‘cutaneous variant’. Br J Haematol. 2004;127:173–183. doi: 10.1111/j.1365-2141.2004.05177.x. - DOI - PubMed
-
- Ponzoni M, Ferreri AJ, Campo E, Facchetti F, Mazzucchelli L, Yoshino T, et al. Definition, diagnosis, and management of intravascular large B-cell lymphoma: proposals and perspectives from an international consensus meeting. J Clin Oncol. 2007;25:3168–3173. doi: 10.1200/JCO.2006.08.2313. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
