

A case of (double) ANCA-negative granulomatosis with polyangiitis (Wegener's)
- PMID: 28509070
- PMCID: PMC5411530
- DOI: 10.1007/s13730-012-0023-4
A case of (double) ANCA-negative granulomatosis with polyangiitis (Wegener's)
Abstract
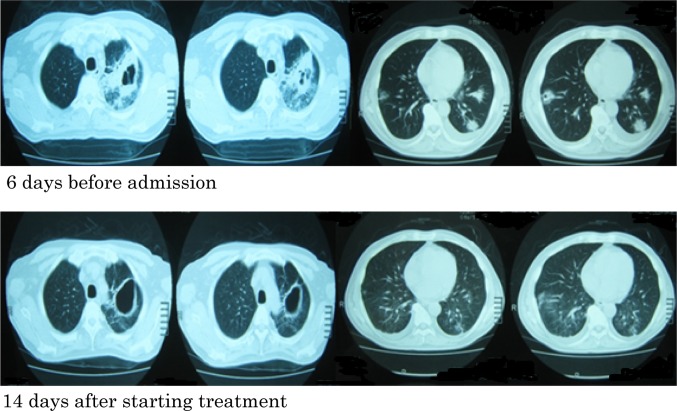
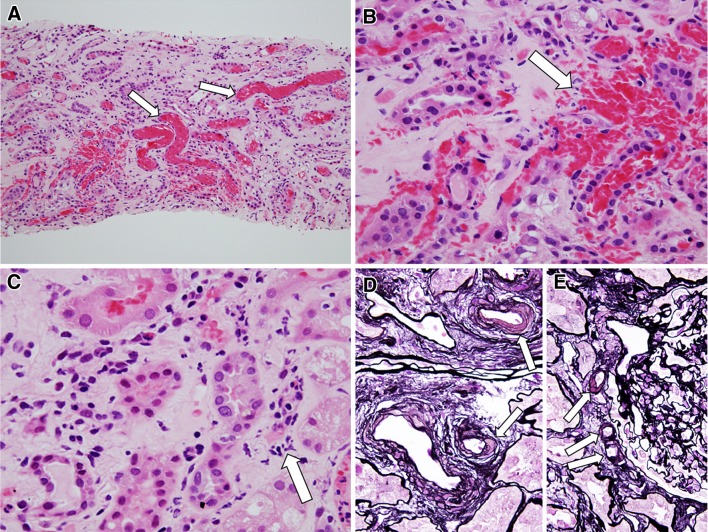
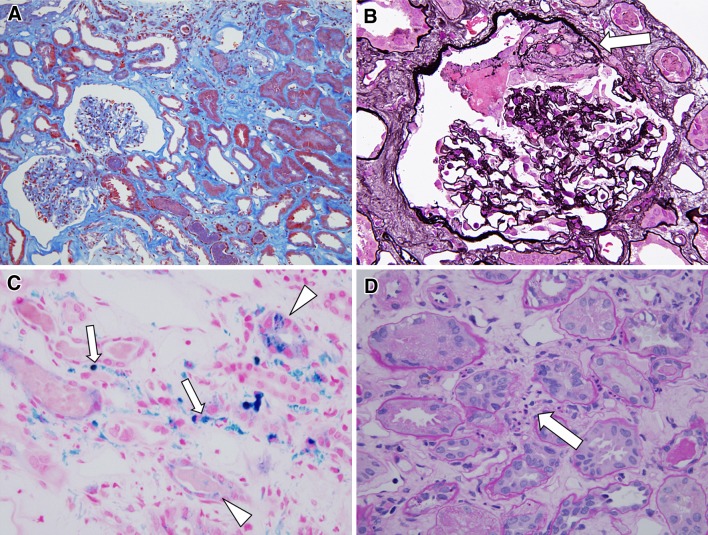
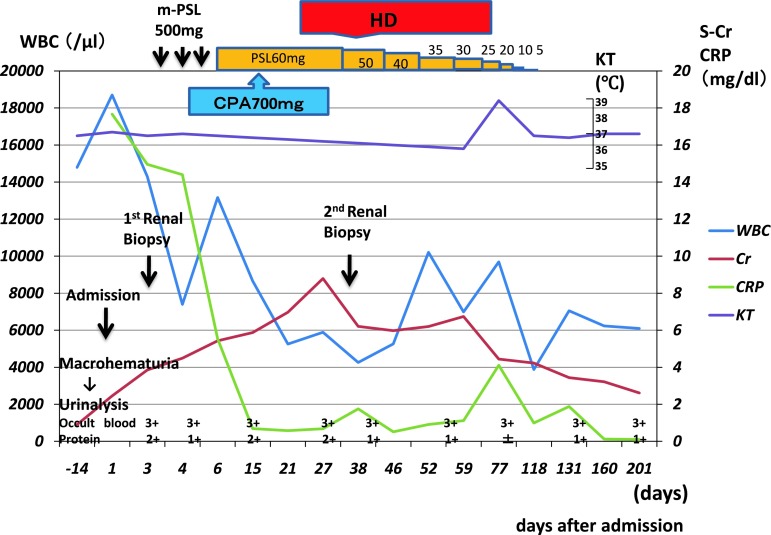
A 60-year-old man had experienced cough, bloody sputum, and a 38 °C fever for 1.5 months. He visited an outpatient clinic and received antibiotics and nonsteroidal anti-inflammatory drugs. However, because the symptoms continued, he visited our hospital. The past medical history included chronic sinusitis, hypertension, and diabetes mellitus. A chest x-ray film and computed tomography showed multiple pulmonary nodules with cavities. Macrohematuria had developed 3 days before admission, and renal function had deteriorated (creatinine, 2.45 mg/dL) in 2 weeks. He was admitted to our hospital because of rapidly progressive glomerulonephritis (RPGN) and multiple pulmonary nodules. On admission, the clinical diagnosis was suspected to be granulomatosis with polyangiitis (Wegener's) (GPA), although tests for proteinase-3 anti-neutrophil cytoplasmic antibody (PR3-ANCA) were negative. Antibiotics were administered for 5 days. After renal biopsy, methylprednisolone pulse therapy and cyclophosphamide pulse therapy were performed. The pathological diagnosis on the basis of the renal biopsy was glomerular and interstitial hemorrhage, possibly associated with vasculitis. After the treatment, the pulmonary symptoms, multiple pulmonary nodules, and severe inflammatory reactions in the peripheral blood were resolved. However, renal dysfunction progressed to end-stage renal disease 1 month after renal biopsy. Hemodialysis was started, and the steroid therapy was continued. During hemodialysis, a second renal biopsy was performed and led to a diagnosis of pauci-immune focal segmental crescentic glomerulonephritis. Renal function gradually recovered, and hemodialysis was discontinued. This case was (double) ANCA-negative GPA which presented prominent glomerular and interstitial hemorrhage, may be associated with small vessel vasculitis, but without active necrotizing and crescentic glomerular lesions, in the rapidly progressive glomerulonephritis.
Keywords: Granulomatosis with polyangiitis (Wegener’s); Proteinase-3 anti-neutrophil cytoplasmic antibody; Rapidly progressive glomerulonephritis.
Figures

References
-
- Finkielman JD, Lee AS, Hummel AM, Viss MA, Jacob GL, Homburger HA, et al. ANCA are detectable in nearly all patients with active severe Wegener’s granulomatosis. Am J Med. 2007;120(7):643–14. - PubMed
-
- Falk RJ, Jennette JC. ANCA small-vessel vasculitis. J Am Soc Nephrol. 1997;8(2):314–322. - PubMed
-
- Hagen EC, Daha MR, Hermans J, Andrassy K, Csernok E, Gaskin G, et al. Diagnostic value of standardized assays for anti-neutrophil cytoplasmic antibodies in idiopathic systemic vasculitis. EC/BCR Project for ANCA Assay Standardization. Kidney Int. 1998;53(3):743–753. doi: 10.1046/j.1523-1755.1998.00807.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
