

Systemic and rapidly progressive light-chain deposition disease initially presenting as tubulointerstitial nephritis
- PMID: 28509073
- PMCID: PMC5413647
- DOI: 10.1007/s13730-012-0026-1
Systemic and rapidly progressive light-chain deposition disease initially presenting as tubulointerstitial nephritis
Abstract
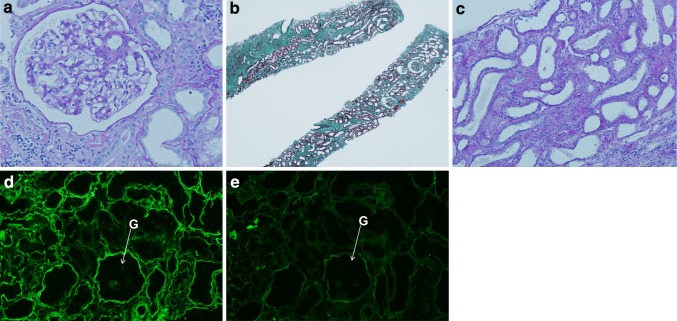
A 42-year-old woman was admitted to a hospital after first-time detection of proteinuria and hematuria during a routine medical check-up. Because her serum creatinine level had rapidly increased from 0.9 to 3.2 mg/dl since measurement 3 months earlier, she was referred to our hospital. Renal biopsy revealed extensive tubular atrophy and interstitial fibrosis with mild leukocyte infiltration. Glomeruli showed minimal changes, and no immunoglobulin or complement deposition was observed by immunofluorescence. Oral prednisolone was commenced under the diagnosis of chronic tubulointerstitial nephritis, and she discharged once. However, its effects were transient; her renal function deteriorated rapidly and hemodialysis was initiated 5 months after her initial check-up. On readmission, urinary Bence-Jones protein κ-type was detected, and examination of bone marrow led to a diagnosis of Bence-Jones κ-type multiple myeloma. Light-chain staining using a renal biopsy specimen obtained 2 months earlier showed κ-light-chain deposition on tubular basement membranes but not glomeruli. Despite undergoing chemotherapy with vincristine, doxirubicin, and dexamethasone, the patient died suddenly from a cardiac arrhythmia. Autopsy showed κ-light-chain deposition in the heart, thyroid, liver, lungs, spleen, and ovaries. Congo red staining yielded negative results. Typical light-chain deposition disease (LCDD) characterized by nodular glomerulosclerosis was observed in the kidneys. This case demonstrates that tubulointerstitial nephritis can be an early pathological variant of LCDD, which may be followed by accelerated and massive light-chain deposition in glomeruli.
Keywords: Cardiac arrhythmia; Cardiac death; Light-chain deposition disease; Monoclonal immunoglobulin deposition disease; Multiple myeloma; Tubulointerstitial nephritis.
Figures


References
-
- Ronco PM, Alyanakian MA, Mougenot B, Aucouturier P. Light chain deposition disease: a model of glomerulosclerosis defined at the molecular level. J Am Soc Nephrol. 2001;12:1558–1565. - PubMed
-
- Lin J, Markowitz GS, Valeri AM, Kambham N, Sherman WH, Appel GB, et al. Renal monoclonal immunoglobulin deposition disease: the disease spectrum. J Am Soc Nephrol. 2001;12:1482–1492. - PubMed
LinkOut - more resources
Full Text Sources
