

Renal-limited vasculitis with elevated levels of multiple antibodies
- PMID: 28509135
- PMCID: PMC5438812
- DOI: 10.1007/s13730-017-0248-3
Renal-limited vasculitis with elevated levels of multiple antibodies
Abstract
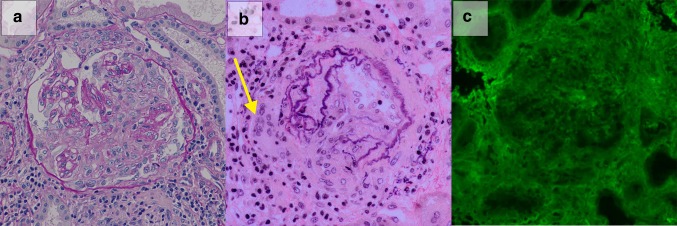
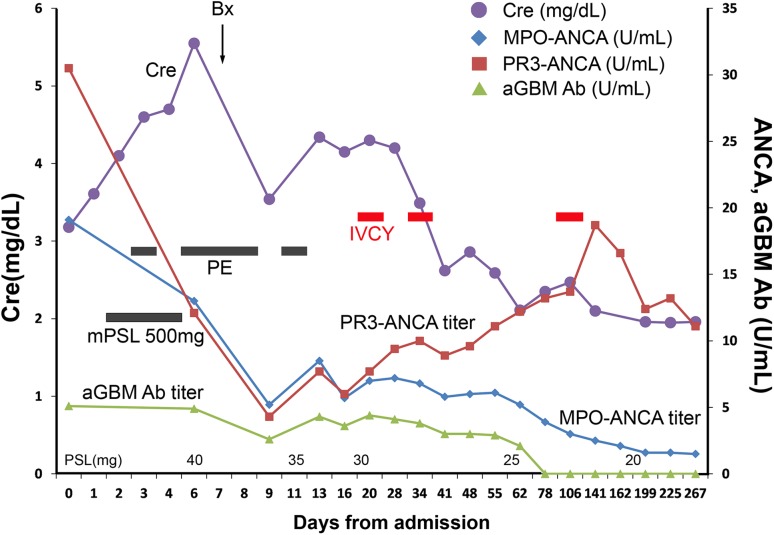
Renal-limited vasculitis (RLV) is a type of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis that presents with crescentic glomerulonephritis with no other organ involvement. Although several studies reported patients with crescentic glomerulonephritis who were dual positive for proteinase 3 (PR3)-ANCA and myeloperoxidase (MPO)-ANCA or ANCA and anti-glomerular basement membrane (GBM) antibody, patients positive for all three antibodies, i.e., triple-positive patients, were rarely reported. We herein report the case of a male with pauci-immune type crescentic glomerulonephritis positive for MPO-ANCA, PR3-ANCA, and anti-GBM antibody. Renal biopsy led to the definitive diagnosis of RLV with pauci-immune-type crescentic glomerulonephritis. Fluorescence immunostaining showed no linear deposition of IgG on GBM, indicating no involvement of anti-GBM associated diseases. Intensive therapy, including prednisolone, plasma exchange, and intravenous cyclophosphamide, was effective. We report the case of triple-positive patient with crescentic glomerulonephritis, who was successfully treated with glucocorticoid, plasma exchange, and cyclophosphamide, suggesting that treatment for RLV in the patient with serological triple antibodies positivity in the absence of linear IgG deposition could benefit from the combination therapy regimen for plasma exchange and primary induction of remission against microscopic polyangiitis.
Keywords: Anti-GBM antibody; Case report; MPO-ANCA; PR3-ANCA.
Conflict of interest statement
Conflict of interest
The authors declare that they have no competing interests.
Ethics and consent to participate
All relevant ethics for the case report and its publication were obtained.
Consent to publish
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Figures

Similar articles
-
Dual anti-neutrophil cytoplasmic antibody-related pauci-immune crescentic glomerulonephritis in a patient with Sjögren's syndrome.Rheumatol Int. 2016 Sep;36(9):1327-34. doi: 10.1007/s00296-016-3520-5. Epub 2016 Jul 6. Rheumatol Int. 2016. PMID: 27384449
-
MPO-ANCA-positive anti-glomerular basement membrane antibody disease successfully treated by plasma exchange and immunosuppressive therapy.Ren Fail. 2011;33(6):626-31. doi: 10.3109/0886022X.2011.581401. Epub 2011 May 20. Ren Fail. 2011. PMID: 21599422
-
[Case of rapidly progressive glomerulonephritis with anti-glomerular basement membrane antibody in the course of MPO-ANCA-associated pachymeningitis].Nihon Jinzo Gakkai Shi. 2009;51(4):490-5. Nihon Jinzo Gakkai Shi. 2009. PMID: 19601559 Japanese.
-
New advances in the pathogenesis of ANCA-associated vasculitides.Clin Exp Rheumatol. 2009 Jan-Feb;27(1 Suppl 52):S108-14. Clin Exp Rheumatol. 2009. PMID: 19646356 Review.
-
Coexistence of anti-glomerular basement membrane antibodies and myeloperoxidase-ANCAs in crescentic glomerulonephritis.Am J Kidney Dis. 2005 Aug;46(2):253-62. doi: 10.1053/j.ajkd.2005.05.003. Am J Kidney Dis. 2005. PMID: 16112043 Review.
Cited by
-
A Fatal Case of Rapidly Progressive Glomerulonephritis With Two Anti-neutrophil Cytoplasmic Antibodies and Anti-glomerular Basement Membrane Antibody: A Description of Autopsy Findings.Cureus. 2023 Aug 26;15(8):e44160. doi: 10.7759/cureus.44160. eCollection 2023 Aug. Cureus. 2023. PMID: 37753026 Free PMC article.
-
From Kidney to Brain: An Uncommon Severe Relapse of Myeloperoxidase Anti-Neutrophil Cytoplasmic Antibody (MPO-ANCA) Vasculitis.Cureus. 2021 Mar 31;13(3):e14205. doi: 10.7759/cureus.14205. Cureus. 2021. PMID: 33936909 Free PMC article.
-
Renal histopathological predictors of end-stage kidney disease in ANCA-associated vasculitis with glomerulonephritis: a single-centre study in Korea.Sci Rep. 2023 Sep 8;13(1):14850. doi: 10.1038/s41598-023-41811-0. Sci Rep. 2023. PMID: 37684336 Free PMC article.
-
A Rare Case of Pulmonary-Renal Syndrome With Triple-Seropositive for Myeloperoxidase-Anti-Neutrophil Cytoplasm Antibody (MPO-ANCA), Proteinase 3 (PR3)-ANCA and Anti-Glomerular Basement Membrane (GBM) Antibodies.J Med Cases. 2021 Oct;12(10):405-410. doi: 10.14740/jmc3742. Epub 2021 Sep 29. J Med Cases. 2021. PMID: 34691337 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
