

Tocilizumab-induced remission of nephrotic syndrome accompanied by secondary amyloidosis and glomerulonephritis in a patient with rheumatoid arthritis
- PMID: 28509209
- PMCID: PMC5418500
- DOI: 10.1007/s13730-014-0127-0
Tocilizumab-induced remission of nephrotic syndrome accompanied by secondary amyloidosis and glomerulonephritis in a patient with rheumatoid arthritis
Abstract
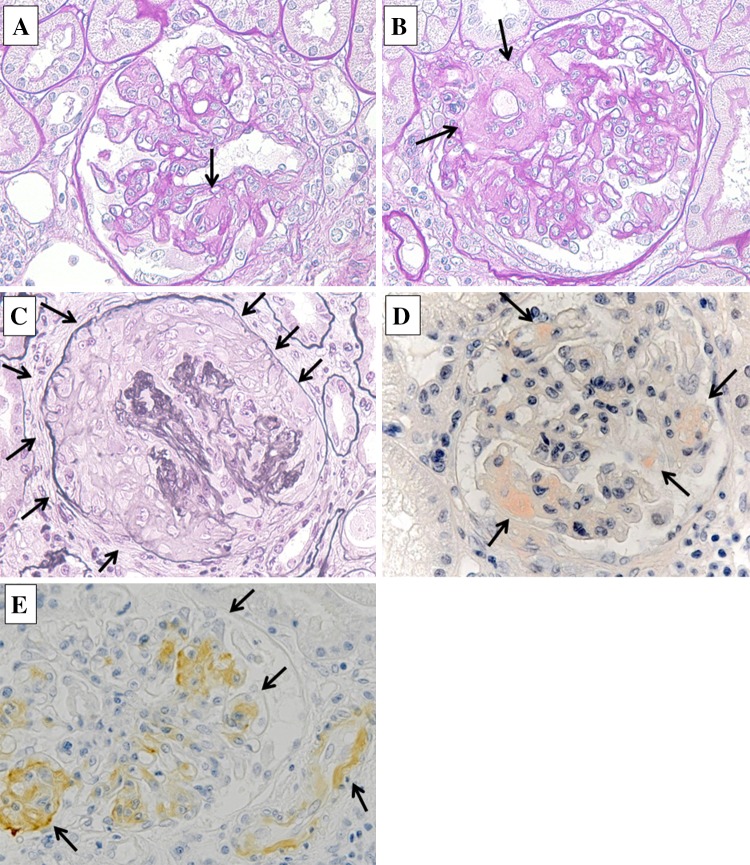
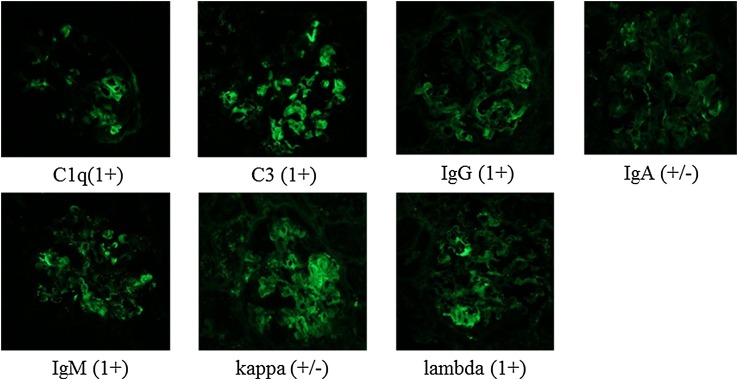
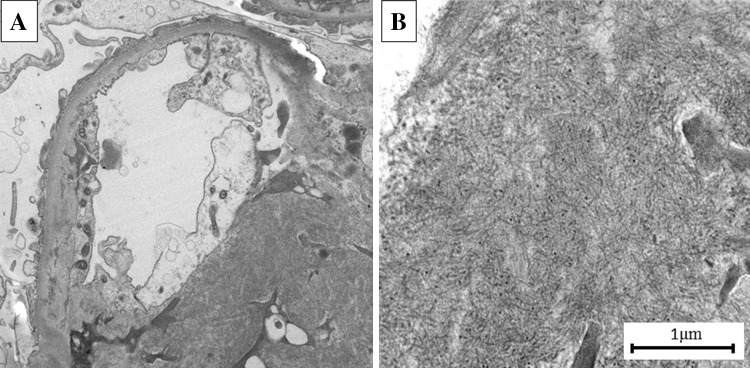
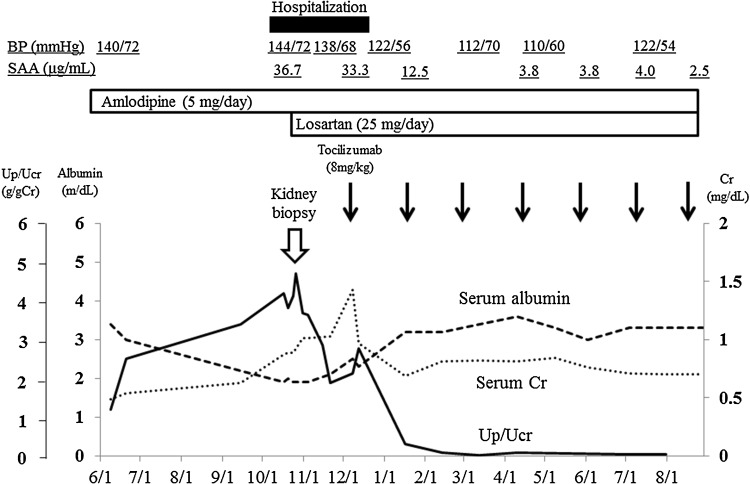
Rheumatoid arthritis (RA) is an autoimmune-mediated systemic disorder that primarily affects the musculoskeletal system. Patients with RA often present with kidney diseases, such as nephrotic syndrome. Causes of nephrotic syndrome include membranous nephropathy, IgA nephropathy and secondary amyloidosis. Recently, biological agents, including anti-tumor necrosis factor alpha and anti-interleukin 6 (IL-6) receptor antibodies, have been used for the treatment of RA. Anti-IL-6 receptor antibody therapy is believed to ameliorate RA-related kidney diseases, as IL-6 plays a central role in the pathogenesis of RA. We, herein, present the case of a patient with RA and related nephrotic syndrome whose proteinuria completely disappeared 1 month after tocilizumab treatment. A light microscopic examination of the pretreatment kidney biopsy specimen showed active glomerulonephritis with fibrocellular crescents and the deposition of amorphous substances stained weakly with hematoxylin-eosin and strongly with the Dylon method. Electron microscopy revealed the accumulation of microtubules ranging from 10 to 20 μm in width, primarily in the mesangial lesion. Amyloid A (AA) protein was positively stained in the mesangial area and vascular wall on immunohistochemistry. The final histologic diagnosis was RA-related glomerulonephritis and secondary AA amyloidosis. This case indicates that biological treatment targeting IL-6 is a promising therapeutic option for the treatment of kidney diseases associated with RA.
Keywords: AA amyloidosis; Glomerulonephritis; Interleukin-6; Nephrotic syndrome; Rheumatoid arthritis; Tocilizumab.
Figures
Similar articles
-
Serum Amyloid A Protein-Associated Kidney Disease: Presentation, Diagnosis, and Management.Kidney Med. 2022 Jun 26;4(8):100504. doi: 10.1016/j.xkme.2022.100504. eCollection 2022 Aug. Kidney Med. 2022. PMID: 35879979 Free PMC article. Review.
-
Turkish experience in rheumatoid arthritis patients with clinical apparent amyloid deposition.Amyloid. 2013 Dec;20(4):245-50. doi: 10.3109/13506129.2013.840576. Epub 2013 Oct 9. Amyloid. 2013. PMID: 24106838
-
[Case of rheumatoid arthritis with various histological lesions of the kidney].Nihon Jinzo Gakkai Shi. 2006;48(2):67-73. Nihon Jinzo Gakkai Shi. 2006. PMID: 16541759 Japanese.
-
Rapid and sustained response to tocilizumab, anti-interleukin-6 receptor antibody, in a patient with nephrotic syndrome secondary to systemic juvenile idiopathic arthritis-related amyloidosis.NDT Plus. 2011 Jun;4(3):178-80. doi: 10.1093/ndtplus/sfr004. Epub 2011 Mar 2. NDT Plus. 2011. PMID: 25984151 Free PMC article.
-
[Renal disorders in rheumatoid arthritis].Nihon Rinsho. 1992 Mar;50(3):576-80. Nihon Rinsho. 1992. PMID: 1588751 Review. Japanese.
Cited by
-
Tocilizumab preserves renal function in rheumatoid arthritis with AA amyloidosis and end-stage kidney disease: Two case reports.Clin Nephrol. 2021 Jan;95(1):54-61. doi: 10.5414/CN109971. Clin Nephrol. 2021. PMID: 33155543 Free PMC article.
-
Targeting inerleukin-6 for renoprotection.Front Immunol. 2024 Dec 11;15:1502299. doi: 10.3389/fimmu.2024.1502299. eCollection 2024. Front Immunol. 2024. PMID: 39723211 Free PMC article. Review.
-
Serum Amyloid A Protein-Associated Kidney Disease: Presentation, Diagnosis, and Management.Kidney Med. 2022 Jun 26;4(8):100504. doi: 10.1016/j.xkme.2022.100504. eCollection 2022 Aug. Kidney Med. 2022. PMID: 35879979 Free PMC article. Review.
-
Collapsing Focal Segmental Glomerulosclerosis and Acute Kidney Injury Associated With Chimeric Antigen Receptor T-Cell (CAR-T) Therapy: A Case Report.Kidney Med. 2021 Aug 9;3(6):1086-1090. doi: 10.1016/j.xkme.2021.06.011. eCollection 2021 Nov-Dec. Kidney Med. 2021. PMID: 34939018 Free PMC article.
-
Use of tocilizumab in amyloid a nephropathy associated with Sweet syndrome: a case report and literature review.CEN Case Rep. 2021 Feb;10(1):23-29. doi: 10.1007/s13730-020-00507-4. Epub 2020 Jul 17. CEN Case Rep. 2021. PMID: 32681397 Free PMC article.
References
-
- Jennette JC, Olson JL, Schwartz MM, Silva FG, editors. Heptinstall’s renal pathology of the kidney. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007. p. 587–92.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
