

A case of secondary focal segmental glomerulosclerosis associated with malignant hypertension
- PMID: 28509227
- PMCID: PMC5413729
- DOI: 10.1007/s13730-012-0041-2
A case of secondary focal segmental glomerulosclerosis associated with malignant hypertension
Abstract
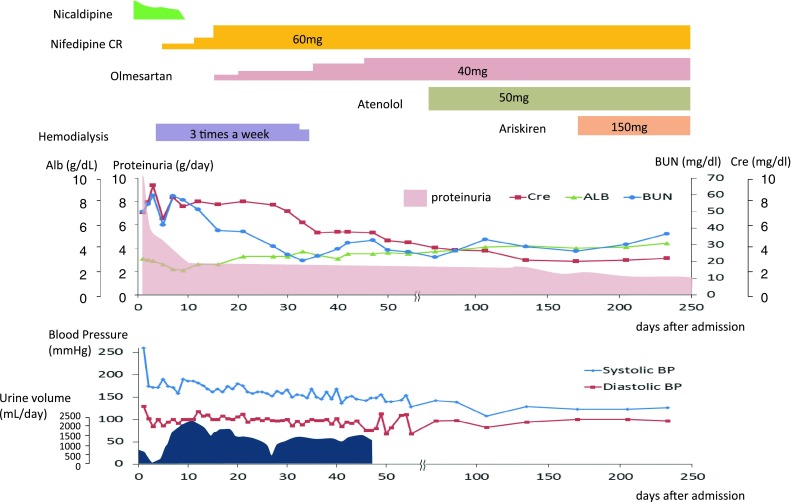
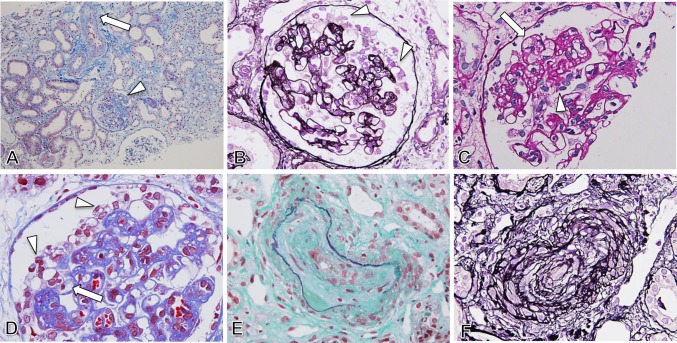
Focal segmental glomerulosclerosis (FSGS) is associated with various clinicopathological conditions, including hypertension. We report here a case of secondary FSGS associated with malignant hypertension. A 33-year-old man with a 1-month history of visual impairment and headache visited the Department of Ophthalmology at our hospital and was found to have hypertensive retinopathy and severe hypertension (230/160 mmHg). He was referred to our department based on suspected renal dysfunction. His blood pressure on admission was 250/130 mmHg. Physical examination and laboratory tests revealed hypertensive cardiac dysfunction, focal brain edema, renal dysfunction (serum creatinine, Cr 7.07 mg/dl, blood urea nitrogen, BUN 49.9 mg/dl), massive proteinuria (10.7 g/day), and thrombotic microangiopathy. Funduscopy showed exudate, hemorrhage, and papilledema. The cause of secondary hypertension could not be identified. He was treated for primary malignant hypertension, but required hemodialysis 3 days after admission due to anuria. Treatment with antihypertensive agents resulted in the gradual recovery of renal function, although heavy proteinuria continued with nephrotic syndrome. Renal biopsy performed 1 month after admission showed features of malignant nephrosclerosis with secondary FSGS. Hemodialysis was discontinued following further improvement in renal function and the most recent laboratory tests showed proteinuria 1.8 g/day and persistent renal dysfunction (BUN 36.5 mg/dl, Cr 3.14 mg/dl). Malignant hypertension may cause various injuries, including glomerular endothelial and epithelial cell injuries in glomerular hypertension and hyperfiltration, increase of the renin-angiotensin-aldosterone system, and endothelial-epithelial interaction, resulting in the development of secondary FSGS and heavy proteinuria.
Keywords: Focal segmental glomerulosclerosis; Hypertensive emergency; Malignant hypertension; Malignant nephrosclerosis; Nephrotic syndrome; Thrombotic microangiopathy.
Figures


Similar articles
-
Complex glomerular pathology of thrombotic microangiopathy and focal segmental glomerulosclerosis forms tumor-like mass in a renal transplant donor with severe renovascular hypertension.CEN Case Rep. 2017 May;6(1):12-17. doi: 10.1007/s13730-016-0235-0. Epub 2016 Sep 26. CEN Case Rep. 2017. PMID: 28509120 Free PMC article.
-
[A case of renovascular hypertension with nephrotic syndrome, accompanied by focal segmental glomerulosclerosis-like lesion in the contralateral kidney].Nihon Jinzo Gakkai Shi. 1991 Oct;33(10):1017-24. Nihon Jinzo Gakkai Shi. 1991. PMID: 1770622 Japanese.
-
Thrombotic microangiopathy as a complication in a patient with focal segmental glomerulosclerosis.Pediatr Nephrol. 2007 Dec;22(12):2125-8. doi: 10.1007/s00467-007-0563-6. Epub 2007 Sep 20. Pediatr Nephrol. 2007. PMID: 17882457
-
Clinicopathological characteristics of obesity-associated focal segmental glomerulosclerosis.Ultrastruct Pathol. 2011 Aug;35(4):176-82. doi: 10.3109/01913123.2011.584657. Epub 2011 Jun 9. Ultrastruct Pathol. 2011. PMID: 21657818 Review.
-
Secondary Focal Segmental Glomerulosclerosis: From Podocyte Injury to Glomerulosclerosis.Biomed Res Int. 2016;2016:1630365. doi: 10.1155/2016/1630365. Epub 2016 Mar 21. Biomed Res Int. 2016. PMID: 27088082 Free PMC article. Review.
Cited by
-
A Case of Rheumatoid Arthritis Presenting with Renal Thrombotic Microangiopathy Probably due to a Combination of Chronic Tacrolimus Arteriolopathy and Severe Hypertension.Case Rep Nephrol. 2019 Mar 6;2019:3923190. doi: 10.1155/2019/3923190. eCollection 2019. Case Rep Nephrol. 2019. PMID: 30963011 Free PMC article.
-
Nephrotic syndrome with focal segmental glomerular lesions unclassified by Columbia classification; Pathology and clinical implication.PLoS One. 2021 Jan 5;16(1):e0244677. doi: 10.1371/journal.pone.0244677. eCollection 2021. PLoS One. 2021. PMID: 33400710 Free PMC article.
-
Effect of hypertension on the long-term prognosis of children with primary focal segmental glomerulosclerosis-a retrospective cohort study.Transl Pediatr. 2023 Feb 28;12(2):155-161. doi: 10.21037/tp-22-649. Epub 2023 Feb 14. Transl Pediatr. 2023. PMID: 36891366 Free PMC article.
-
Complex glomerular pathology of thrombotic microangiopathy and focal segmental glomerulosclerosis forms tumor-like mass in a renal transplant donor with severe renovascular hypertension.CEN Case Rep. 2017 May;6(1):12-17. doi: 10.1007/s13730-016-0235-0. Epub 2016 Sep 26. CEN Case Rep. 2017. PMID: 28509120 Free PMC article.
-
Histopathological and Clinical Findings of Biopsy-Proven Focal and Segmental Glomerulosclerosis: A Retrospective Study.Cureus. 2022 Mar 11;14(3):e23083. doi: 10.7759/cureus.23083. eCollection 2022 Mar. Cureus. 2022. PMID: 35419217 Free PMC article.
References
-
- Rosei EA, Salvetti M, Farsang C. Treatment of hypertensive urgencies and emergencies. Blood Press. 2006;15:255–256. - PubMed
-
- Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mitsuyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshima H, Umemura S, Ishimitsu T, Rakugi H, Japanese Society of Hypertension Committee The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009) Hypertens Res. 2009;32:3–107. - PubMed
-
- Olson JL. Renal disease caused by hypertension. In: Jennette JC, Olson JL, Schwartz MM, Silva FG, editors. Heptinstall’s pathology of the kidney. 6. Philadelphia: Lippincott Williams and Wilkins; 2007. pp. 937–990.
-
- D’Agati VD, Jennette JC, Silva FG. Hypertensive nephrosclerosis, renal artery stenosis, and atheroembolization. In: D’Agati VD, Jennette JC, Silva FG, editors. Atlas of nontumor pathology: non-neoplastic kidney diseases. Washington, DC: American Registry of Pathology; 2005. pp. 425–546.
LinkOut - more resources
Full Text Sources
