

Mizoribine as a safe and effective combined maintenance therapy with prednisolone for anti-neutrophil cytoplasmic antibody-associated vasculitis in a hemodialysis patient
- PMID: 28509286
- PMCID: PMC5418497
- DOI: 10.1007/s13730-012-0050-1
Mizoribine as a safe and effective combined maintenance therapy with prednisolone for anti-neutrophil cytoplasmic antibody-associated vasculitis in a hemodialysis patient
Abstract
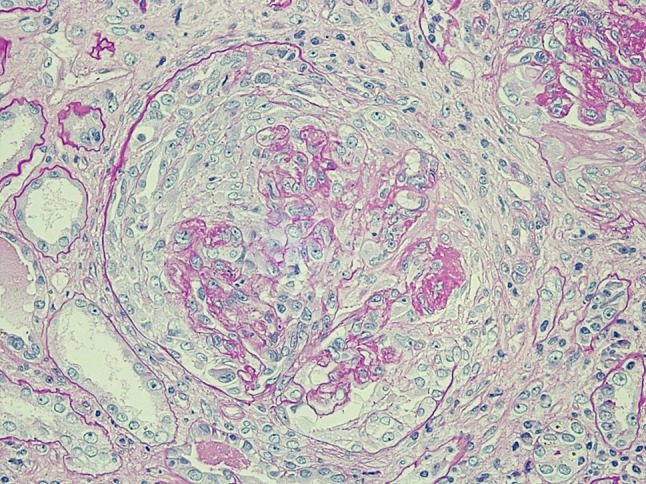
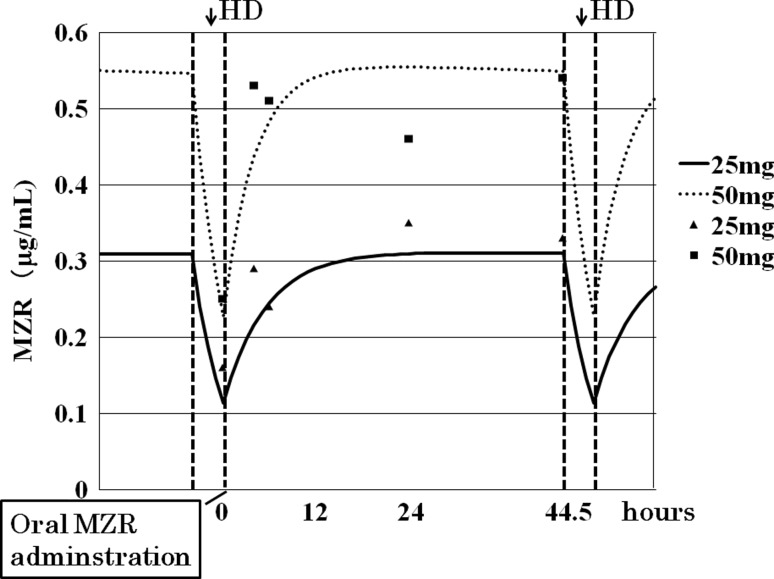
A 77-year-old man developed severe renal insufficiency due to proteinase 3 anti-neutrophil cytoplasmic antibody (PR3-ANCA)-associated vasculitis, and was started on hemodialysis (HD). Because his renal insufficiency appeared to be irreversible, he was maintained on oral prednisolone (PSL) at 5 mg/day. However, a disease flare-up with alveolar hemorrhage occurred. Serology revealed elevated levels of PR3-ANCA and C-reactive protein (CRP). The patient was given pulse therapy with a quarter dose of methylprednisolone (m-PSL) (250 mg, 3 days), followed by oral PSL at 15 mg/day. As a supplemental treatment, he was given 25 mg of mizoribine (MZR) immediately after each HD session. Subsequently, the levels of PR3-ANCA and CRP decreased, and the alveolar hemorrhage resolved. The dose of MZR to be given was determined by measuring the patient's serum concentrations of MZR at various time points after the HD session. The maintenance dose of MZR was finally set at 50 mg. At present, the oral PSL dosage has been tapered to 10 mg/day, and the patient has achieved a state of remission without any side effects.
Keywords: Hemodialysis; Mizoribine; Proteinase 3 anti-neutrophil cytoplasmic antibody-associated vasculitis; Pulmonary hemorrhage.
Figures


References
-
- Ishikawa H. Mizolibine and mycophenolate mofetil. Curr Med Chem. 1999;6:575–97. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
