

Proliferative glomerulonephritis with monoclonal IgG2κ deposit successfully treated with steroids: a case report and review of the literature
- PMID: 28509293
- PMCID: PMC5411552
- DOI: 10.1007/s13730-013-0064-3
Proliferative glomerulonephritis with monoclonal IgG2κ deposit successfully treated with steroids: a case report and review of the literature
Abstract
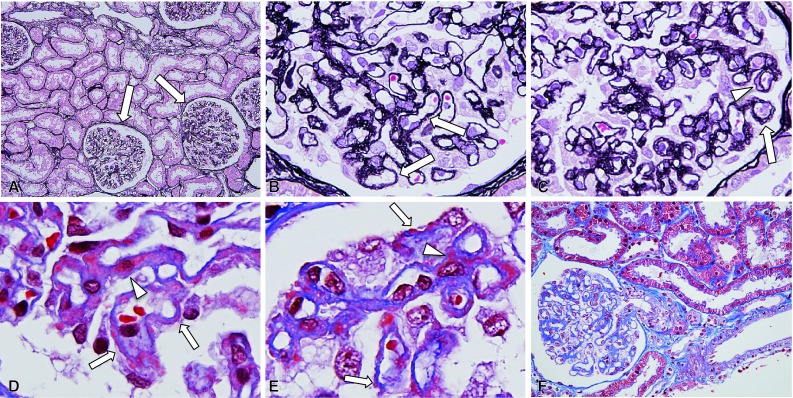
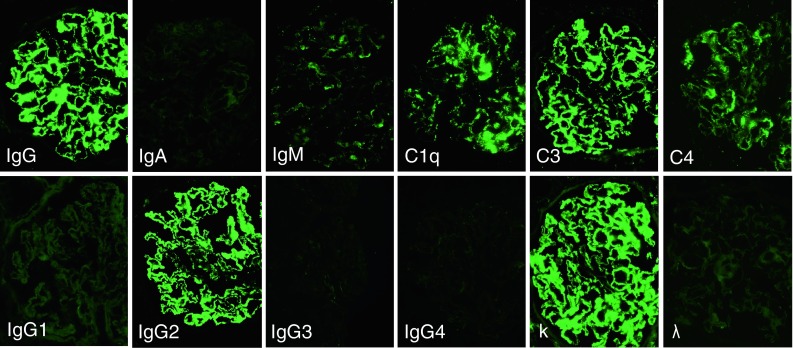
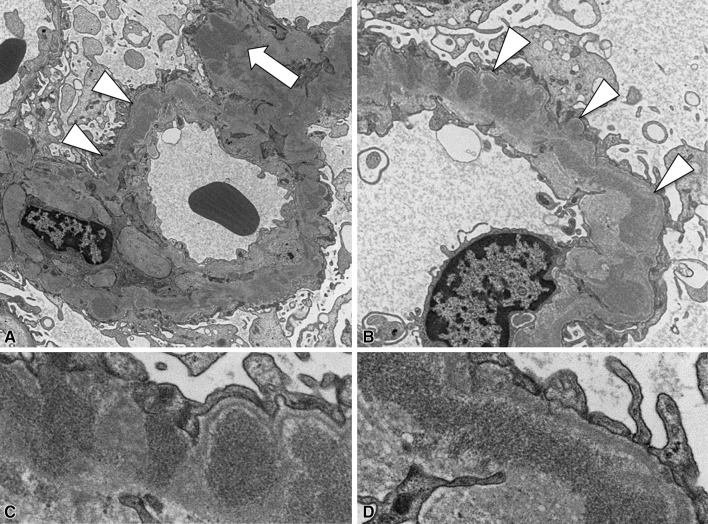
A novel form of glomerular injury with monoclonal immunoglobulin (Ig) IgG deposition, termed "proliferative glomerulonephritis (GN) with monoclonal IgG deposits" (PGNMID), is a recently described entity. PGNMID presents with various histological patterns, such as membranoproliferative GN, endocapillary proliferative GN and membranous nephropathy (MN). The deposits are composed of monoclonal immunoglobulin, most commonly IgG3 and occasionally IgG2. At present, the clinical significance of each IgG subclass and the morphological patterns of glomerular injury have not been fully investigated due to the limited number of PGNMID cases reported. The patient was a 27-year-old woman presenting with a mild degree of proteinuria and no other physical or serological abnormalities. Monoclonal Ig could not be identified in her serum or urine. Renal biopsy found features of MN with deposition of monoclonal IgG2κ. Electron microscopy examination revealed non-organised electron-dense deposits predominantly in subepithelial locations. Based on a diagnosis of PGNMID, she was treated with prednisolone and proteinuria significantly decreased in less than 4 weeks. Although the clinical outcomes of PGNMID remain to be defined, MN features may possibly be a sign of favourable prognosis-a hypothesis supported by recent reports. The absence of advanced chronic damage in the kidney, such as glomerulosclerosis or tubulointerstitial fibrosis, may also have contributed to the favourable outcome in the present case. Further studies on additional PGNMID cases that allow the correlation of morphological features and IgG subclasses with clinical outcomes are needed in order to confirm our findings and further solidify the clinical aspects of this new disease entity.
Keywords: Membranous nephropathy; Monoclonal IgG; Proliferative glomerulonephritis; Steroid.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
