

Genetics and its potential to improve type 1 diabetes care
- PMID: 28509690
- PMCID: PMC6107086
- DOI: 10.1097/MED.0000000000000347
Genetics and its potential to improve type 1 diabetes care
Abstract
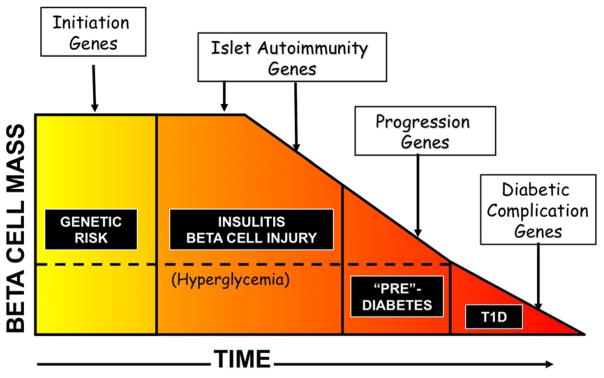
Purpose of review: The genetic basis of type 1 diabetes (T1D) is being characterized through DNA sequence variation and cell type specificity. This review discusses the current understanding of the genes and variants implicated in risk of T1D and how genetic information can be used in prediction, intervention and components of clinical care.
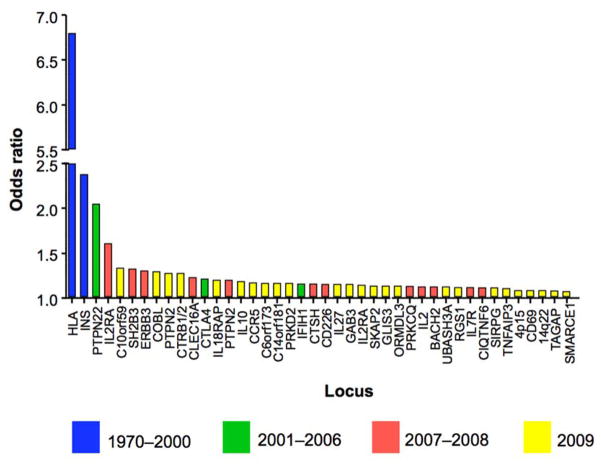
Recent findings: Fine mapping and functional studies has provided resolution of the heritable basis of T1D risk, incorporating novel insights on the dominant role of human leukocyte antigen (HLA) genes as well as the lesser impact of non-HLA genes. Evaluation of T1D-associated single nucleotide polymorphisms (SNPs), there is enrichment of genetic effects restricted to specific immune cell types (CD4 and CD8 T cells, CD19 B cells and CD34 stem cells), suggesting pathways to improved prediction. In addition, T1D-associated SNPs have been used to generate genetic risk scores (GRS) as a tool to distinguish T1D from type 2 diabetes (T2D) and to provide prediagnostic data to target those for autoimmunity screening (e.g. islet autoantibodies) as a prelude for continuous monitoring and entry into intervention trials.
Summary: Genetic susceptibility accounts for nearly one-half of the risk for T1D. Although the T1D-associated SNPs in white populations account for nearly 90% of the genetic risk, with high sensitivity and specificity, the low prevalence of T1D makes the T1D GRS of limited utility. However, identifying those with highest genetic risk may permit early and targeted immune monitoring to diagnose T1D months prior to clinical onset.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Rich SS. Mapping genes in diabetes. Genetic epidemiological perspective Diabetes. 1990;39(11):1315–1319. - PubMed
-
- Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States, 2014. Atlanta, GA: U.S. Department of Health and Human Services; 2014.
-
- Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet. 2001;358(9277):221–229. - PubMed
-
- Nerup J, Platz P, Andersen OO, et al. HL-A antigens and diabetes mellitus. Lancet. 1974;2(7885):864–866. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
