

Identification of novel risk factors for community-acquired Clostridium difficile infection using spatial statistics and geographic information system analyses
- PMID: 28510584
- PMCID: PMC5433765
- DOI: 10.1371/journal.pone.0176285
Identification of novel risk factors for community-acquired Clostridium difficile infection using spatial statistics and geographic information system analyses
Abstract
Background: The rate of community-acquired Clostridium difficile infection (CA-CDI) is increasing. While receipt of antibiotics remains an important risk factor for CDI, studies related to acquisition of C. difficile outside of hospitals are lacking. As a result, risk factors for exposure to C. difficile in community settings have been inadequately studied.
Main objective: To identify novel environmental risk factors for CA-CDI.
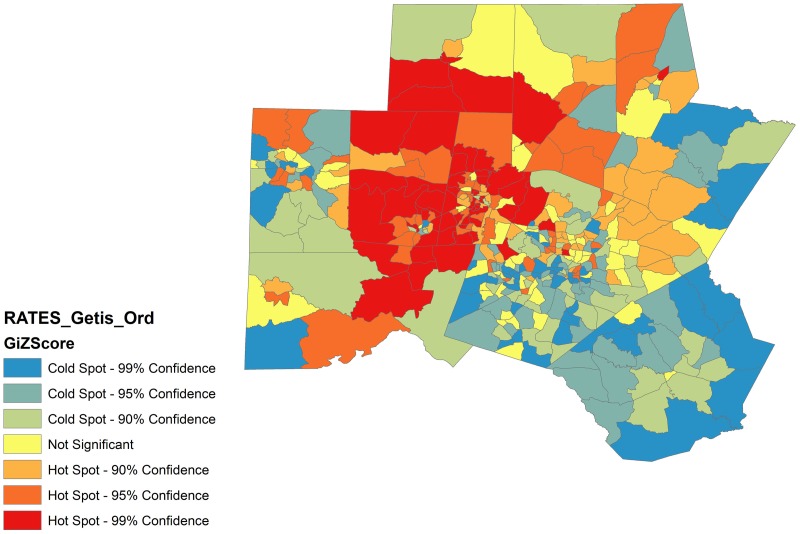
Methods: We performed a population-based retrospective cohort study of patients with CA-CDI from 1/1/2007 through 12/31/2014 in a 10-county area in central North Carolina. 360 Census Tracts in these 10 counties were used as the demographic Geographic Information System (GIS) base-map. Longitude and latitude (X, Y) coordinates were generated from patient home addresses and overlaid to Census Tracts polygons using ArcGIS; ArcView was used to assess "hot-spots" or clusters of CA-CDI. We then constructed a mixed hierarchical model to identify environmental variables independently associated with increased rates of CA-CDI.
Results: A total of 1,895 unique patients met our criteria for CA-CDI. The mean patient age was 54.5 years; 62% were female and 70% were Caucasian. 402 (21%) patient addresses were located in "hot spots" or clusters of CA-CDI (p<0.001). "Hot spot" census tracts were scattered throughout the 10 counties. After adjusting for clustering and population density, age ≥ 60 years (p = 0.03), race (<0.001), proximity to a livestock farm (0.01), proximity to farming raw materials services (0.02), and proximity to a nursing home (0.04) were independently associated with increased rates of CA-CDI.
Conclusions: Our study is the first to use spatial statistics and mixed models to identify important environmental risk factors for acquisition of C. difficile and adds to the growing evidence that farm practices may put patients at risk for important drug-resistant infections.
Conflict of interest statement
Figures

References
-
- Miller BA, Chen LF, Sexton DJ, Anderson DJ. Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile Infection and of healthcare-associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol. 2011;32(4):387–90. Epub 2011/04/05. 10.1086/659156 - DOI - PubMed
-
- Centers for Disease Control and Prevention. Antibiotic Resistance Threats in the United States, 20132013 09/18/2013. http://www.cdc.gov/drugresistance/threat-report-2013/.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
