

Self reported outcomes and adverse events after medical abortion through online telemedicine: population based study in the Republic of Ireland and Northern Ireland
- PMID: 28512085
- PMCID: PMC5431774
- DOI: 10.1136/bmj.j2011
Self reported outcomes and adverse events after medical abortion through online telemedicine: population based study in the Republic of Ireland and Northern Ireland
Abstract
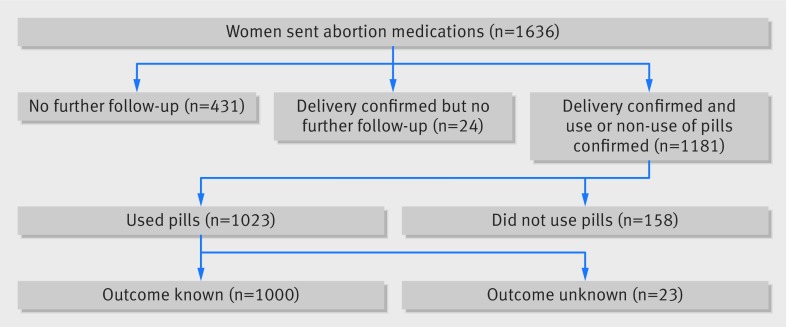
Objectives To assess self reported outcomes and adverse events after self sourced medical abortion through online telemedicine.Design Population based study.Setting Republic of Ireland and Northern Ireland, where abortion is unavailable through the formal healthcare system except in a few restricted circumstances.Population 1000 women who underwent self sourced medical abortion through Women on Web (WoW), an online telemedicine service, between 1 January 2010 and 31 December 2012.Main outcome measures Successful medical abortion: the proportion of women who reported ending their pregnancy without surgical intervention. Rates of adverse events: the proportion who reported treatment for adverse events, including receipt of antibiotics and blood transfusion, and deaths reported by family members, friends, or the authorities. Care seeking for symptoms of potential complications: the frequency with which women reported experiencing symptoms of a potentially serious complication and the proportion who reported seeking medical attention as advised.Results In 2010-12, abortion medications (mifepristone and misoprostol) were sent to 1636 women and follow-up information was obtained for 1158 (71%). Among these, 1023 women confirmed use of the medications, and follow-up information was available for 1000. At the time women requested help from WoW, 781 (78%) were <7 weeks pregnant and 219 (22%) were 7-9 weeks pregnant. Overall, 94.7% (95% confidence interval 93.1% to 96.0%) reported successfully ending their pregnancy without surgical intervention. Seven women (0.7%, 0.3% to 1.5%) reported receiving a blood transfusion, and 26 (2.6%, 1.7% to 3.8%) reported receiving antibiotics (route of administration (IV or oral) could not be determined). No deaths resulting from the intervention were reported by family, friends, the authorities, or the media. Ninety three women (9.3%, 7.6% to 11.3%) reported experiencing any symptom for which they were advised to seek medical advice, and, of these, 87 (95%, 87.8% to 98.2%) sought attention. None of the five women who did not seek medical attention reported experiencing an adverse outcome.Conclusions Self sourced medical abortion using online telemedicine can be highly effective, and outcomes compare favourably with in clinic protocols. Reported rates of adverse events are low. Women are able to self identify the symptoms of potentially serious complications, and most report seeking medical attention when advised. Results have important implications for women worldwide living in areas where access to abortion is restricted.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare grants from the Society of Family Planning (ARAA) and infrastructure support from the National Institutes of Health (JT and ARAA); RG is founder and director of Women on Web, ID is a prescribing physician for Women on Web, JT serves on the Board of the Women on Web Foundation; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Abortion by telemedicine: an equitable option for Irish women.BMJ. 2017 May 16;357:j2237. doi: 10.1136/bmj.j2237. BMJ. 2017. PMID: 28512132 Free PMC article.
References
-
- Center for Reproductive Rights. World abortion laws. http://worldabortionlaws.com/
-
- Kassebaum NJ, Bertozzi-Villa A, Coggeshall MS, et al. Global, regional, and national levels and causes of maternal mortality during 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014;384:980-1004. 10.1016/S0140-6736(14)60696-6 pmid:24797575. - DOI - PMC - PubMed
-
- Grimes DA, Benson J, Singh S, et al. Unsafe abortion: the preventable pandemic. Lancet 2006;368:1908-19. 10.1016/S0140-6736(06)69481-6 pmid:17126724. - DOI - PubMed
-
- Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health 2014;2:e323-33. 10.1016/S2214-109X(14)70227-X pmid:25103301. - DOI - PubMed
-
- Costa SH. Commercial availability of misoprostol and induced abortion in Brazil. Int J Gynaecol Obstet 1998;63(Suppl 1):S131-9. 10.1016/S0020-7292(98)00195-7 pmid:10075223. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical