

Cell death biomarker M65 is a useful indicator of liver inflammation and fibrosis in chronic hepatitis B: A cross-sectional study of diagnostic accuracy
- PMID: 28514295
- PMCID: PMC5440132
- DOI: 10.1097/MD.0000000000006807
Cell death biomarker M65 is a useful indicator of liver inflammation and fibrosis in chronic hepatitis B: A cross-sectional study of diagnostic accuracy
Abstract
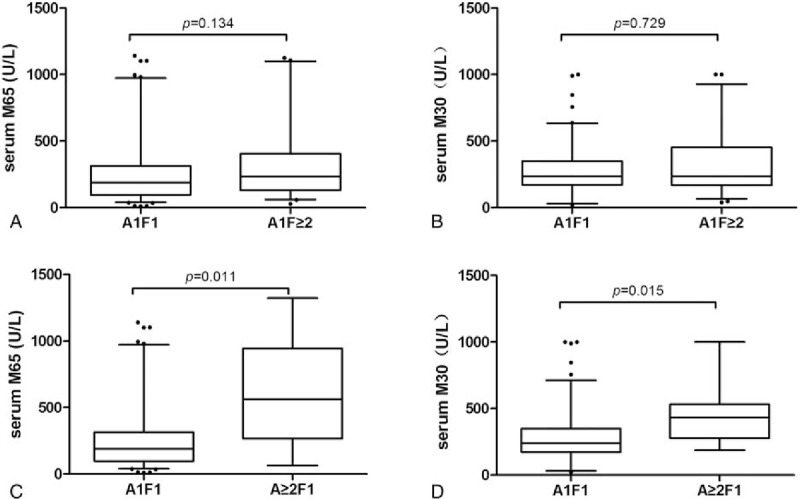
Cell death markers, M65 and M30, have been suggested to be sensitive markers of liver inflammation and fibrosis in nonalcoholic fatty liver disease and chronic hepatitis C. Our aim was to investigate whether these markers were useful in diagnosing liver inflammation and fibrosis in chronic hepatitis B (CHB).We examined 186 patients with CHB; 18 sex- and age-matched healthy subjects were controls. The blood samples were collected from CHB patients within 1 week before or after liver biopsy. According to METAVIR score system, liver inflammation was graded from A0 to A3, and fibrosis from F0 to F4.Serum M65 and M30 levels were in parallel with the grades of liver inflammation. M65, not M30, increased significantly in patients with severe inflammation and normal alanine aminotransferase. M65 is one of the independent predictors of severe liver inflammation (≥A2). The levels of M65 and M30 levels significantly increased in parallel with the degree of inflammation in F1 patients, whereas they showed no statistical difference between different stages of fibrosis in A1 patients.Serum M65 is a useful indicator of liver inflammation in CHB patients. Serum M65, not M30, is valuable in the grading of liver fibrosis.
Conflict of interest statement
The authors report no conflicts of interest.
Figures



Similar articles
-
Prognostic value of M30/M65 for outcome of hepatitis B virus-related acute-on-chronic liver failure.World J Gastroenterol. 2014 Mar 7;20(9):2403-11. doi: 10.3748/wjg.v20.i9.2403. World J Gastroenterol. 2014. PMID: 24605039 Free PMC article.
-
Clinical significance of serum Ck18-M65 and M30 levels in patients with chronic hepatitis B combined with nonalcoholic steatohepatitis and liver fibrosis.Medicine (Baltimore). 2024 Jun 7;103(23):e38342. doi: 10.1097/MD.0000000000038342. Medicine (Baltimore). 2024. PMID: 38847670 Free PMC article.
-
The expression of serum M30 and M65 in chronic hepatitis B patients with non-alcoholic fatty liver disease.Eur Rev Med Pharmacol Sci. 2015 Nov;19(21):4123-9. Eur Rev Med Pharmacol Sci. 2015. PMID: 26592838
-
Accuracy of cytokeratin 18 (M30 and M65) in detecting non-alcoholic steatohepatitis and fibrosis: A systematic review and meta-analysis.PLoS One. 2020 Sep 11;15(9):e0238717. doi: 10.1371/journal.pone.0238717. eCollection 2020. PLoS One. 2020. PMID: 32915852 Free PMC article.
-
Serum markers of liver fibrosis: combining the BIPED classification and the neo-epitope approach in the development of new biomarkers.Dis Markers. 2010;28(1):15-28. doi: 10.3233/DMA-2010-0678. Dis Markers. 2010. PMID: 20164543 Free PMC article. Review.
Cited by
-
Association of cell death mechanisms and fibrosis in visceral white adipose tissue with pathological alterations in the liver of morbidly obese patients with NAFLD.Adipocyte. 2021 Dec;10(1):558-573. doi: 10.1080/21623945.2021.1982164. Adipocyte. 2021. PMID: 34743657 Free PMC article.
-
Presence of Liver Inflammation in Asian Patients With Chronic Hepatitis B With Normal ALT and Detectable HBV DNA in Absence of Liver Fibrosis.Hepatol Commun. 2022 Apr;6(4):855-866. doi: 10.1002/hep4.1859. Epub 2021 Nov 15. Hepatol Commun. 2022. PMID: 34783181 Free PMC article.
-
Cell-free DNA Release in the Plasma of Patients with Cardiac Disease is Associated with Cell Death Processes.Indian J Clin Biochem. 2023 Jan;38(1):67-72. doi: 10.1007/s12291-022-01034-y. Epub 2022 Apr 21. Indian J Clin Biochem. 2023. PMID: 36684502 Free PMC article.
-
Molecular Biomarkers in Drug-Induced Liver Injury: Challenges and Future Perspectives.Front Pharmacol. 2020 Jan 30;10:1667. doi: 10.3389/fphar.2019.01667. eCollection 2019. Front Pharmacol. 2020. PMID: 32082163 Free PMC article. Review.
-
Comparison between chronic hepatitis B patients with untreated immune-tolerant phase vs. those with virological response by antivirals.Sci Rep. 2019 Feb 21;9(1):2508. doi: 10.1038/s41598-019-39043-2. Sci Rep. 2019. PMID: 30792468 Free PMC article.
References
-
- McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology 2009;49:45–55. - PubMed
-
- Lai M, Hyatt BJ, Nasser I, et al. The clinical significance of persistently normal ALT in chronic hepatitis B infection. J Hepatol 2007;47:760–7. - PubMed
-
- Kumar M, Sarin SK, Hissar S, et al. Virologic and histologic features of chronic hepatitis B virus-infected asymptomatic patients with persistently normal ALT. Gastroenterology 2008;134:1376–84. - PubMed
-
- Chen EQ, Huang FH, He LL, et al. Histological changes in Chinese chronical hepatitis B patients with ALT lower than two times upper limits of normal. Dig Dis Sci 2010;55:432–7. - PubMed
-
- Forns X, Ampurdanes S, Llovet JM, et al. Identification of chronic hepatitis C patients without hepatic fibrosis by a simple predictive model. Hepatology 2002;36:986–92. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
