

Clinicopathological features and differential diagnosis of aggressive angiomyxoma of the female pelvis: 5 case reports and literature review
- PMID: 28514296
- PMCID: PMC5440133
- DOI: 10.1097/MD.0000000000006820
Clinicopathological features and differential diagnosis of aggressive angiomyxoma of the female pelvis: 5 case reports and literature review
Abstract
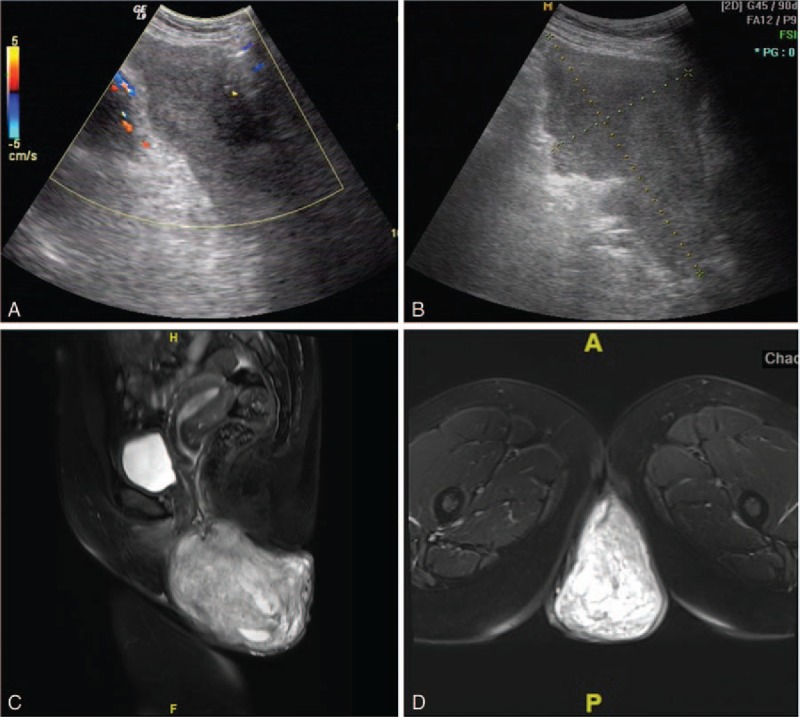
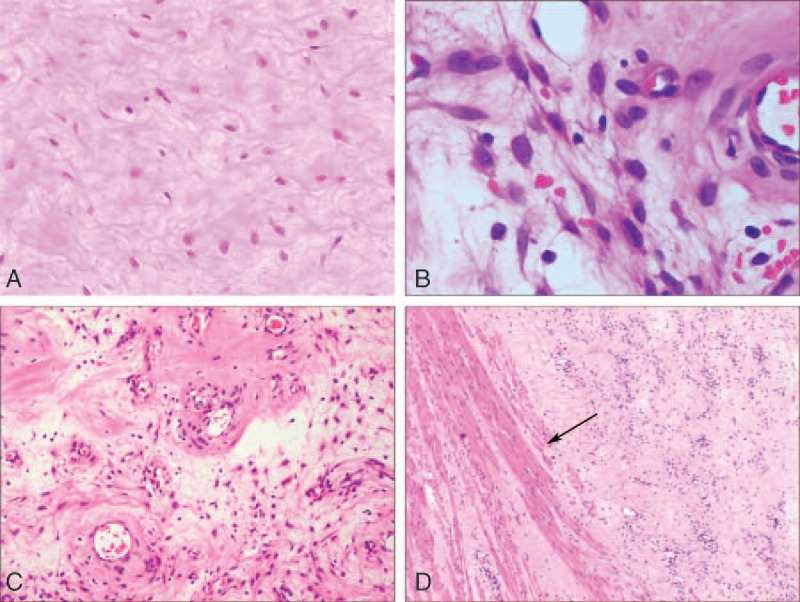
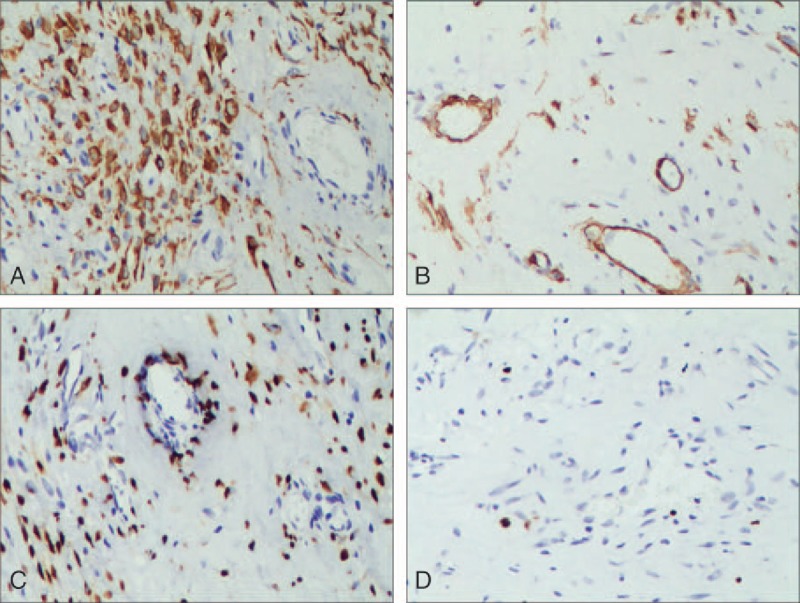
Aggressive angiomyxoma (AAM) is a rare mesenchymal tumor that usually occurs in the pelvis and perineum of young females. AAM can simulate Bartholin's gland cyst, abscess, lipoma, simple labial cyst, or other pelvic soft tissue tumors. Here we present five cases of AAM with mean age of 42. The patients mainly presented slow-growing mass in the abdomen and perineum (3 cases in the pelvis, 1 in the vulva, and 1 in the buttock). Color Doppler flow imaging revealed blood flow for the 3 pelvic lesions. Enhanced computed tomography and magnetic resonance imaging of the other 2 cases showed the typical "swirled" or "layered" structure characteristic. Through the pathological examination, its positivity to estrogen and progesterone receptors can justify enlargement and recurrence, confirming the tumor is AAM. All 5 patients underwent local tumor resection. Two patients recurred 8 and 15 months after surgery, respectively. The longest follow-up was 42 months. Although few cases are reported, early recognition demands high index of suspicion for both gynaecologists and pathologists. Wide surgical excision with tumor free margins is the basis of curative treatment. Adjuvant therapy may be necessary for residual or recurrent tumors. Long-term follow-up is recommended.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Fletcher C, Bridge J, Hogendoorn P, et al. World Health Organization Classification of Tumours of Soft Tissue and Bone. 4th ed.Lyon: IARC Press; 2013.
-
- Outwater EK, Marchetto BE, Wagner BJ, et al. Aggressive angiomyxoma: findings on CT and MR imaging. AJR Am J Roentgenol 1999;172:435–8. - PubMed
-
- Steeper TA, Rosai J. Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am J Surg Pathol 1983;7:463–75. - PubMed
-
- Tariq R, Hasnain S, Siddiqui MT, et al. Aggressive angiomyxoma: swirled configuration on ultrasound and MR imaging. J Pak Med Assoc 2014;64:345–8. - PubMed
-
- Li X, Ye Z. Aggressive angiomyxoma of the pelvis and perineum: a case report and review of the literature. Abdom Imaging 2011;36:739–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
