

Cardiopulmonary Resuscitation Training Disparities in the United States
- PMID: 28515114
- PMCID: PMC5524119
- DOI: 10.1161/JAHA.117.006124
Cardiopulmonary Resuscitation Training Disparities in the United States
Abstract
Background: Bystander cardiopulmonary resuscitation (CPR) is associated with increased survival from cardiac arrest, yet bystander CPR rates are low in many communities. The overall prevalence of CPR training in the United States and associated individual-level disparities are unknown. We sought to measure the national prevalence of CPR training and hypothesized that older age and lower socioeconomic status would be independently associated with a lower likelihood of CPR training.
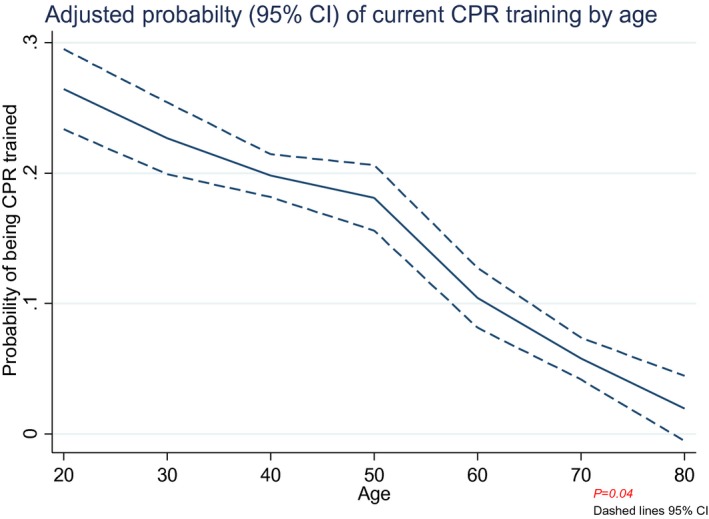
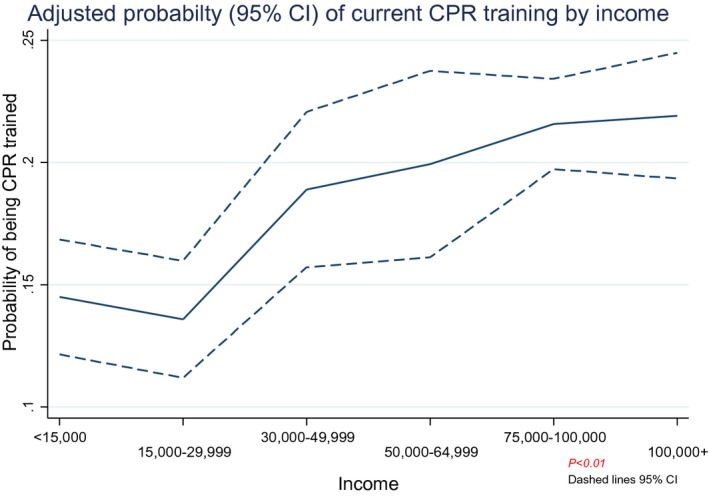
Methods and results: We administered a cross-sectional telephone survey to a nationally representative adult sample. We assessed the demographics of individuals trained in CPR within 2 years (currently trained) and those who had been trained in CPR at some point in time (ever trained). The association of CPR training and demographic variables were tested using survey weighted logistic regression. Between September 2015 and November 2015, 9022 individuals completed the survey; 18% reported being currently trained in CPR, and 65% reported training at some point previously. For each year of increased age, the likelihood of being currently CPR trained or ever trained decreased (currently trained: odds ratio, 0.98; 95% CI, 0.97-0.99; P<0.01; ever trained: OR, 0.99; 95% CI, 0.98-0.99; P=0.04). Furthermore, there was a greater then 4-fold difference in odds of being currently CPR trained from the 30-39 to 70-79 year old age groups (95% CI, 0.10-0.23). Factors associated with a lower likelihood of CPR training were lesser educational attainment and lower household income (P<0.01 for each of these variables).
Conclusions: A minority of respondents reported current training in CPR. Older age, lesser education, and lower income were associated with reduced likelihood of CPR training. These findings illustrate important gaps in US CPR education and suggest the need to develop tailored CPR training efforts to address this variability.
Keywords: cardiopulmonary resuscitation; education; education surveillance; educational campaigns; sudden cardiac arrest.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Regions With Low Rates of Bystander Cardiopulmonary Resuscitation (CPR) Have Lower Rates of CPR Training in Victoria, Australia.J Am Heart Assoc. 2017 Jun 5;6(6):e005972. doi: 10.1161/JAHA.117.005972. J Am Heart Assoc. 2017. PMID: 28584073 Free PMC article.
-
Association of race and socioeconomic status with automatic external defibrillator training prevalence in the United States.Resuscitation. 2018 Jun;127:100-104. doi: 10.1016/j.resuscitation.2018.03.037. Epub 2018 Apr 7. Resuscitation. 2018. PMID: 29631005
-
Australia's awareness of cardiac arrest and rates of CPR training: results from the Heart Foundation's HeartWatch survey.BMJ Open. 2020 Jan 6;10(1):e033722. doi: 10.1136/bmjopen-2019-033722. BMJ Open. 2020. PMID: 31911523 Free PMC article.
-
Socioeconomic disparities in layperson CPR training within a large U.S. city.Resuscitation. 2019 Aug;141:13-18. doi: 10.1016/j.resuscitation.2019.05.038. Epub 2019 Jun 8. Resuscitation. 2019. PMID: 31185261
-
Improving bystander cardiopulmonary resuscitation.Curr Opin Crit Care. 2011 Jun;17(3):219-24. doi: 10.1097/MCC.0b013e32834697d8. Curr Opin Crit Care. 2011. PMID: 21499092 Review.
Cited by
-
Multi-Community Cardiopulmonary Resuscitation Education by Medical Students.Cureus. 2020 Jun 15;12(6):e8647. doi: 10.7759/cureus.8647. Cureus. 2020. PMID: 32685315 Free PMC article.
-
Awareness, Knowledge, and Attitudes Regarding Basic Life Support Among the Population With Relatives Suffering From Heart Diseases in the Al-Qassim Region, Saudi Arabia.Cureus. 2022 Nov 15;14(11):e31530. doi: 10.7759/cureus.31530. eCollection 2022 Nov. Cureus. 2022. PMID: 36532927 Free PMC article.
-
Awareness, Knowledge, and Attitudes Regarding Cardiopulmonary Resuscitation in Case of Cardiac Arrest among the Population in the Jazan Region, Saudi Arabia.Ann Afr Med. 2024 Apr 1;23(2):118-124. doi: 10.4103/aam.aam_25_23. Epub 2023 Oct 10. Ann Afr Med. 2024. PMID: 39028158 Free PMC article.
-
Knowledge of non-healthcare individuals towards cardiopulmonary resuscitation: a cross-sectional study in Riyadh City, Saudi Arabia.Int J Emerg Med. 2021 Feb 10;14(1):11. doi: 10.1186/s12245-021-00335-y. Int J Emerg Med. 2021. PMID: 33568064 Free PMC article.
-
Characteristics and outcomes of out-of-hospital-cardiac-arrest in rural and suburban areas of Sindh, Pakistan: A cross-sectional study.Resusc Plus. 2024 Dec 12;21:100840. doi: 10.1016/j.resplu.2024.100840. eCollection 2025 Jan. Resusc Plus. 2024. PMID: 39807285 Free PMC article.
References
-
- Hasselqvist‐Ax I, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg P, Ringh M, Jonsson M, Axelsson C, Lindqvist J, Karlsson T, Svensson L. Early cardiopulmonary resuscitation in out‐of‐hospital cardiac arrest. N Engl J Med. 2015;372:2307–2315. - PubMed
-
- Iwami T, Kawamura T, Hiraide A, Berg RA, Hayashi Y, Nishiuchi T, Kajino K, Yonemoto N, Yukioka H, Sugimoto H, Kakuchi H, Sase K, Yokoyama H, Nonogi H. Effectiveness of bystander‐initiated cardiac‐only resuscitation for patients with out‐of‐hospital cardiac arrest. Circulation. 2007;116:2900–2907. - PubMed
-
- Malta Hansen C, Kragholm K, Pearson DA, Tyson C, Monk L, Myers B, Nelson D, Dupre ME, Fosbol EL, Jollis JG, Strauss B, Anderson ML, McNally B, Granger CB. Association of bystander and first‐responder intervention with survival after out‐of‐hospital cardiac arrest in North Carolina, 2010–2013. JAMA. 2015;314:255–264. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
