

Anti-Glomerular Basement Membrane Disease
- PMID: 28515156
- PMCID: PMC5498345
- DOI: 10.2215/CJN.01380217
Anti-Glomerular Basement Membrane Disease
Abstract
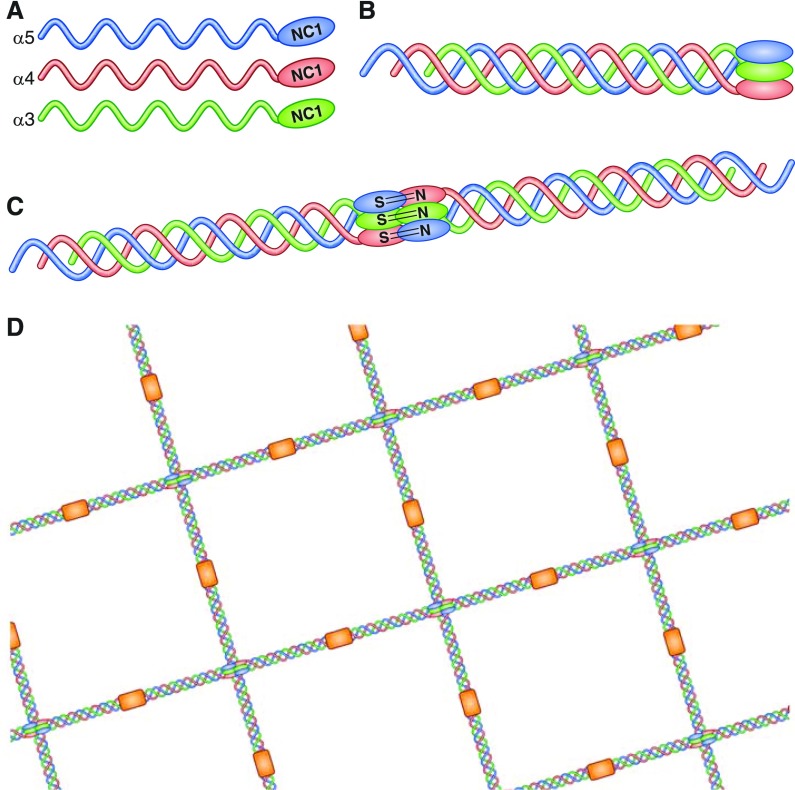
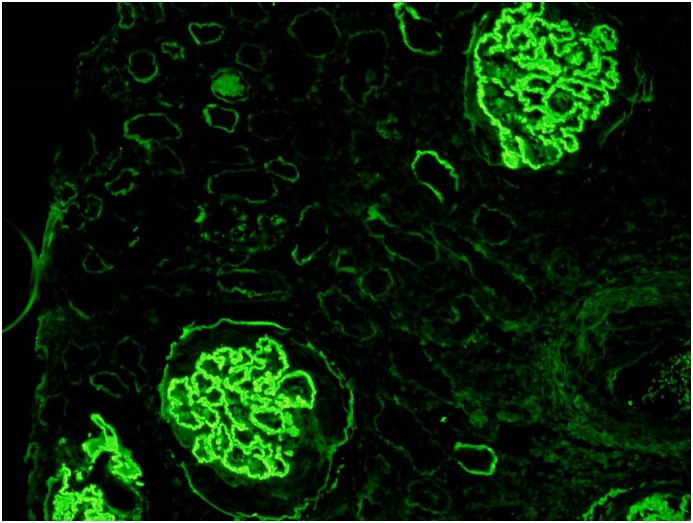
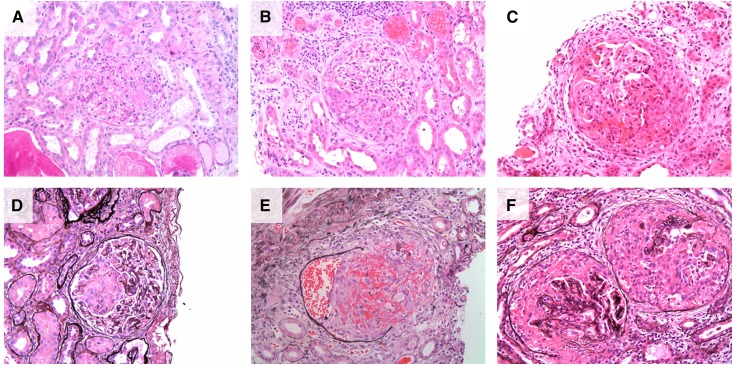
Anti-glomerular basement membrane (anti-GBM) disease is a rare small vessel vasculitis that affects the capillary beds of the kidneys and lungs. It is an archetypic autoimmune disease, caused by the development of directly pathogenic autoantibodies targeting a well characterized autoantigen expressed in the basement membranes of these organs, although the inciting events that induce the autoimmune response are not fully understood. The recent confirmation of spatial and temporal clustering of cases suggests that environmental factors, including infection, may trigger disease in genetically susceptible individuals. The majority of patients develop widespread glomerular crescent formation, presenting with features of rapidly progressive GN, and 40%-60% will have concurrent alveolar hemorrhage. Treatment aims to rapidly remove pathogenic autoantibody, typically with the use of plasma exchange, along with steroids and cytotoxic therapy to prevent ongoing autoantibody production and tissue inflammation. Retrospective cohort studies suggest that when this combination of treatment is started early, the majority of patients will have good renal outcome, although presentation with oligoanuria, a high proportion of glomerular crescents, or kidney failure requiring dialysis augur badly for renal prognosis. Relapse and recurrent disease after kidney transplantation are both uncommon, although de novo anti-GBM disease after transplantation for Alport syndrome is a recognized phenomenon. Copresentation with other kidney diseases such as ANCA-associated vasculitis and membranous nephropathy seems to occur at a higher frequency than would be expected by chance alone, and in addition atypical presentations of anti-GBM disease are increasingly reported. These observations highlight the need for future work to further delineate the immunopathogenic mechanisms of anti-GBM disease, and how to better refine and improve treatments, particularly for patients presenting with adverse prognostic factors.
Keywords: Anti-Glomerular Basement Membrane Disease; Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis; Autoantibodies; Autoantigens; Autoimmunity; Capillaries; Glomerular Basement Membrane; Glomerulonephritis; Hereditary; Humans; Immunology and pathology; Inflammation; Membranous; Nephritis; Plasma Exchange; Plasmapheresis; Prognosis; Recurrence; Renal Insufficiency; Retrospective Studies; glomerulonephritis; kidney; kidney transplantation; renal dialysis; vasculitis.
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, Hoffman GS, Jayne DR, Kallenberg CG, Lamprecht P, Langford CA, Luqmani RA, Mahr AD, Matteson EL, Merkel PA, Ozen S, Pusey CD, Rasmussen N, Rees AJ, Scott DG, Specks U, Stone JH, Takahashi K, Watts RA: 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 65: 1–11, 2013 - PubMed
-
- Stanton MC, Tange JD: Goodpasture’s syndrome (pulmonary haemorrhage associated with glomerulonephritis). Australas Ann Med 7: 132–144, 1958 - PubMed
-
- Goodpasture E: The significance of certain pulmonary lesions in relation to the etiology of influenza. Am J Med Sci 158: 863–870, 1919 - PubMed
-
- Scheer RL, Grossman MA: Immune aspects of the glomerulonephritis associated with pulmonary hemorrhage. Ann Intern Med 60: 1009–1021, 1964
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
