

Preliminary experience with 4K ultra-high definition endoscope: analysis of pros and cons in skull base surgery
- PMID: 28516968
- PMCID: PMC5463515
- DOI: 10.14639/0392-100X-1684
Preliminary experience with 4K ultra-high definition endoscope: analysis of pros and cons in skull base surgery
Abstract
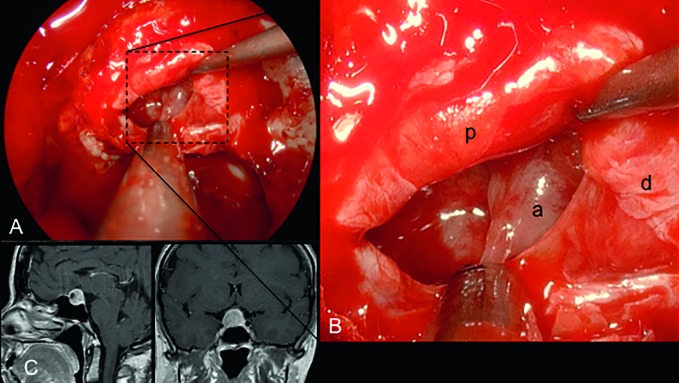
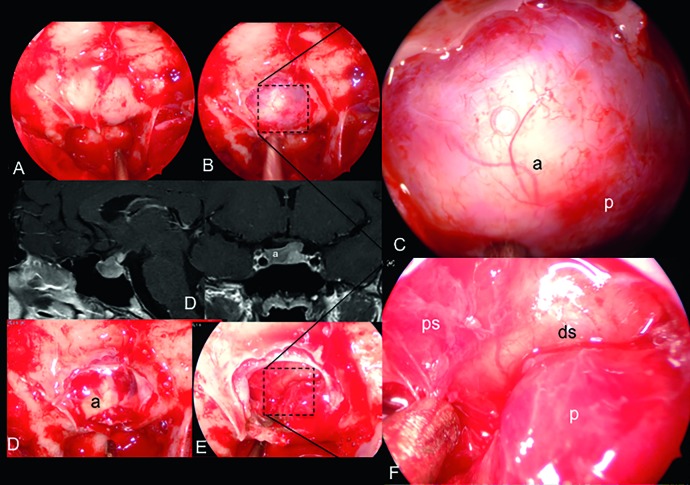
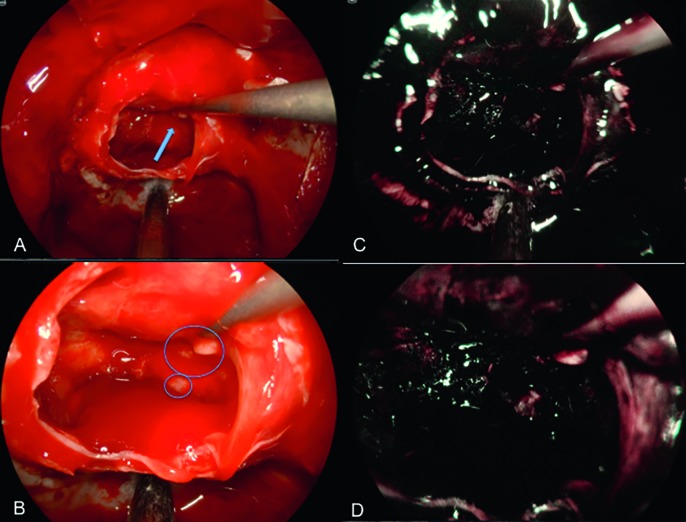
During the last two decades endoscopic skull base surgery observed a continuous technical and technological development 3D endoscopy and ultra High Definition (HD) endoscopy have provided great advances in terms of visualisation and spatial resolution. Ultra-high definition (UHD) 4K systems, recently introduced in the clinical practice, will shape next steps forward especially in skull base surgery field. Patients were operated on through transnasal transsphenoidal endoscopic approaches performed using Olympus NBI 4K UHD endoscope with a 4 mm 0° Ultra Telescope, 300 W xenon lamp (CLV-S400) predisposed for narrow band imaging (NBI) technology connected through a camera head to a high-quality control unit (OTV-S400 - VISERA 4K UHD) (Olympus Corporation, Tokyo, Japan). Two screens are used, one 31" Monitor - (LMD-X310S) and one main ultra-HD 55" screen optimised for UHD image reproduction (LMD-X550S). In selected cases, we used a navigation system (Stealthstation S7, Medtronic, Minneapolis, MN, US). We evaluated 22 pituitary adenomas (86.3% macroadenomas; 13.7% microadenomas). 50% were not functional (NF), 22.8% GH, 18.2% ACTH, 9% PRL-secreting. Three of 22 were recurrences. In 91% of cases we achieved total removal, while in 9% near total resection. A mean follow-up of 187 days and average length of hospitalisation was 3.09 ± 0.61 days. Surgical duration was 128.18± 30.74 minutes. We experienced only 1 case of intraoperative low flow fistula with no further complications. None of the cases required any post- or intraoperative blood transfusion. The visualisation and high resolution of the operative field provided a very detailed view of all anatomical structures and pathologies allowing an improvement in safety and efficacy of the surgical procedure. The operative time was similar to the standard 2D HD and 3D procedures and the physical strain was also comparable to others in terms of ergonomics and weight.
Negli ultimi venti anni la chirurgia endoscopica del basicranio ha osservato continui sviluppi tecnici e tecnologici. L’endoscopia 3D e l’ alta definizione (HD) 4K hanno fornito grandi vantaggi in termini di visualizzazione e di risoluzione spaziale. L’ ultra HD 4K, recentemente introdotta nella pratica clinica, determinerà i prossimi passi soprattutto nella chirurgica endoscopica del basicranio. I pazienti sono stati operati attraverso un approccio transnasale transfenoidale endoscopico, utilizzando un endoscopio Olympus NBI 4K UHD con ottica 4 mm 0 ° Ultra Telescope, lampada allo xeno 300 W (CLV-S400) predisposto per la tecnologia narrow band imaging (NBI) collegato con una videocamera ad un alta qualità unità di controllo (OTV-S400 - VISERA 4K UHD) (Olympus, Tokyo, Giappone). Due schermi, un 31 “Monitor - (LMD-X310S) e quello principale ultra-HD 55” a pollici ottimizzati per la riproduzione immagini UHD (LMD-X550S). In casi selezionati abbiamo usato un sistema di navigazione (Stealthstation S7, Medtronic, Minneapolis, MN, Stati Uniti). Abbiamo valutato 22 adenomi ipofisari (86,3% macroadenomi; 13,7% microadenomi). Il 50% non erano secernenti (NS), 22,8% GH, 18,2% ACTH, 9% PRLsecernenti. 3/22 erano recidive. Nel 91% dei casi abbiamo raggiunto la rimozione totale, mentre nel 9% la resezione subtotale. Un followup medio di 187 giorni, durata media del ricovero era 3,09 ± 0,61 giorni. Tempo chirurgico 128,18 ± 30,74 minuti. Abbiamo avuto solo 1 caso di fistola intraoperatoria a basso flusso senza ulteriori complicazioni nel follow up. Il 100% dei casi non ha richiesto emotrasfusione. La visualizzazione e l’alta risoluzione del campo operatorio hanno fornito una vista dettagliata di tutte le strutture anatomiche e patologie e permesso il miglioramento della sicurezza e l’efficacia della procedura chirurgica. Il tempo operatorio è stato simile a quello dell’endoscopio HD standard 2D e 3D, come la fatica fisica era paragonabile ad altri in termini di ergonomicità e peso.
Keywords: 4K; Endoscopic sinus surgery; Endoscopy; Skull base; Ultra-high definition.
© Copyright by Società Italiana di Otorinolaringologia e Chirurgia Cervico-Facciale, Rome, Italy.
Figures
Similar articles
-
Comparative Evaluation of 3-Dimensional High Definition and 2-Dimensional 4-K Ultra-High Definition Endoscopy Systems in Endonasal Skull Base Surgery.Oper Neurosurg. 2020 Sep 1;19(3):281-287. doi: 10.1093/ons/opz426. Oper Neurosurg. 2020. PMID: 31960059
-
Ultra-high definition (8K UHD) endoscope: our first clinical success.Springerplus. 2016 Aug 30;5(1):1445. doi: 10.1186/s40064-016-3135-z. eCollection 2016. Springerplus. 2016. PMID: 27652021 Free PMC article.
-
Impact of 4K ultra-high-definition endoscope in pituitary surgery: analysis of a comparative institutional case series.J Neurosurg Sci. 2022 Oct;66(5):425-433. doi: 10.23736/S0390-5616.20.04875-4. Epub 2020 Feb 10. J Neurosurg Sci. 2022. PMID: 32043848
-
Transnasal endoscopy-assisted skull base surgery.Ann Otol Rhinol Laryngol Suppl. 2006 Sep;196:45-53. doi: 10.1177/00034894061150s908. Ann Otol Rhinol Laryngol Suppl. 2006. PMID: 17040018 Review.
-
The awake endoscope-guided sealant technique with fibrin glue in the treatment of postoperative cerebrospinal fluid leak after extended transsphenoidal surgery: technical note.World Neurosurg. 2014 Sep-Oct;82(3-4):e479-85. doi: 10.1016/j.wneu.2013.01.017. Epub 2013 Jan 8. World Neurosurg. 2014. PMID: 23313259 Review.
Cited by
-
Two- and three-dimensional endoscopic endonasal surgery of large and giant pituitary adenomas-outcome analysis of a series of 62 patients from a single pituitary center.Neurosurg Rev. 2023 Jun 26;46(1):150. doi: 10.1007/s10143-023-02050-z. Neurosurg Rev. 2023. PMID: 37358696
-
Safety considerations in laparoscopic surgery: A narrative review.World J Gastrointest Endosc. 2022 Jan 16;14(1):1-16. doi: 10.4253/wjge.v14.i1.1. World J Gastrointest Endosc. 2022. PMID: 35116095 Free PMC article. Review.
-
Management of cerebrospinal fluid leak: the importance of multidisciplinary approach.Acta Otorhinolaryngol Ital. 2021 Apr;41(Suppl. 1):S18-S29. doi: 10.14639/0392-100X-suppl.1-41-2021-02. Acta Otorhinolaryngol Ital. 2021. PMID: 34060517 Free PMC article.
-
Multidisciplinary approach to the craniovertebral junction. Historical insights, current and future perspectives in the neurosurgical and otorhinolaryngological alliance.Acta Otorhinolaryngol Ital. 2021 Apr;41(Suppl. 1):S51-S58. doi: 10.14639/0392-100X-suppl.1-41-2021-05. Acta Otorhinolaryngol Ital. 2021. PMID: 34060520 Free PMC article.
-
Performance of three-dimensional and ultra-high-definition (4K) technology in laparoscopic surgery: A systematic review and meta-analysis.J Minim Access Surg. 2022 Apr-Jun;18(2):167-175. doi: 10.4103/jmas.jmas_122_21. J Minim Access Surg. 2022. PMID: 35313429 Free PMC article. Review.
References
-
- Maier H, Heer G, Ortac A, et al. Capturing and displaying microscopic images used in medical diagnostics and forensic science using 4K video resolution – an application in higher education. J Microsc. 2015;260:175–179. - PubMed
-
- Cappabianca P, Cavallo LM, Esposito F, et al. Endoscopic endonasal transsphenoidal surgery: procedure, endoscopic equipment and instrumentation. Childs Nerv Syst. 2004;20:796–801. - PubMed
-
- Arens C, Betz C, Kraft M, et al. Narrow band imaging for early diagnosis of epithelial dysplasia and microinvasive tumors in the upper aerodigestive tract. HNO. 2017;65(Suppl 1):5–12. - PubMed
-
- Akutsu N, Taniguchi M, Kohmura E. Visualization of the normal pituitary gland during the endoscopic endonasal removal of pituitary adenoma by narrow band imaging. Acta Neurochir (Wien) 2016;158:1977–1981. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
