

Sialendoscopy for salivary stones: principles, technical skills and therapeutic experience
- PMID: 28516972
- PMCID: PMC5463517
- DOI: 10.14639/0392-100X-1599
Sialendoscopy for salivary stones: principles, technical skills and therapeutic experience
Abstract
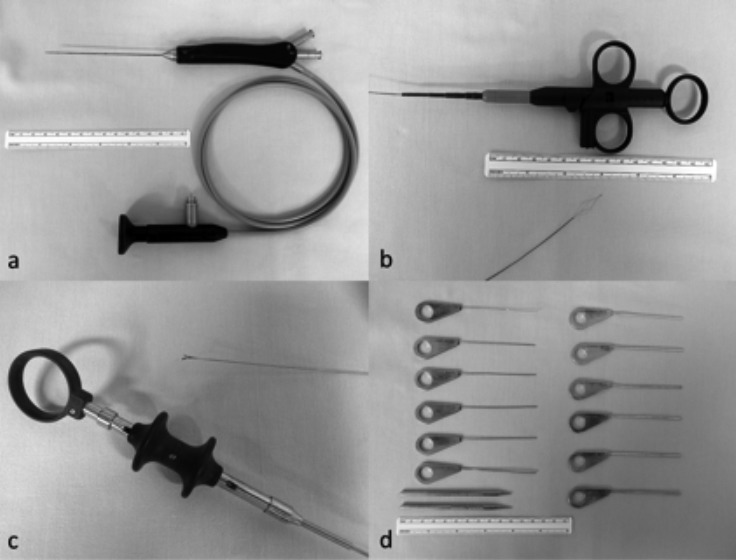
Obstructive sialadenitis is the most common non-neoplastic disease of the salivary glands, and sialendoscopy is increasingly used in both diagnosis and treatment, associated in selected cases with endoscopic laser lithotripsy. Sialendoscopy is also used for combined minimally invasive external and endoscopic approaches in patients with larger and proximal stones that would require excessively long laser procedures. The present paper reports on the technical experience from the Ear, Nose and Throat Unit of the Sant'Orsola-Malpighi Hospital of Bologna, and from the Department of Otorhinolaryngology of the University Hospital of Cagliari, Italy, including the retrospective analysis of the endoscopic and endoscopic assisted procedures performed on 48 patients (26 females and 22 males; median age 45.3; range 8-83 years) treated for chronic obstructive sialadenitis at the University Hospital of Cagliari from November 2010 to April 2016. The results from the Sant'Orsola-Malpighi Hospital of Bologna have been previously published. The technical aspects of sialendoscopy are carefully described. The retrospective analysis of the University Hospital of Cagliari shows that the disease was unilateral in 40 patients and bilateral in 8; a total of 56 major salivary glands were treated (22 submandibular glands and 34 parotids). Five patients underwent bilateral sialendoscopy for juvenile recurrent parotitis. 10 patients were treated for non-lithiasic obstructive disease. In 33 patients (68.75%) the obstruction was caused by salivary stones (bilateral parotid lithiasis in 1 case). Only 8 patients needed a sialectomy (5 submandibular glands and 3 parotids). The conservative approach to obstructive sialadenitis is feasible and can be performed either purely endoscopically or in a combined modality, with a high percentage of success. The procedure must be performed with dedicated instrumentation by a skilled surgeon after proper training since minor to major complications can be encountered. Sialectomy should be the "extrema ratio" after failure of a conservative approach.
La scialoadenite cronica ostruttiva rappresenta una delle più frequenti patologie non-neoplastiche delle ghiandole salivari e la scialoendoscopia è sempre più utilizzata nella sua diagnosi e nel suo trattamento, associata o meno con la litotripsia laser. La scialoendoscopia può essere inoltre associata ad approcci esterni mini-invasivi nelle litiasi troppo voluminose per essere rimosse con un approccio unicamente endoscopico. Il presente articolo riporta l’esperienza delle Cliniche Otorinolaringoiatriche dell’Ospedale Sant’Orsola-Malpighi di Bologna e dell’Azienda Ospedaliero Universitaria di Cagliari, Italia. È stata eseguita un’analisi retrospettiva su 48 pazienti (26 femmine, 22 maschi; età media di 45,3 anni; range 8-83 anni) trattati per patologia cronica ostruttiva delle ghiandole salivari maggiori mediante procedure chirurgiche endoscopiche o combinate da novembre 2010 ad aprile 2016 presso l’Azienda-Ospedaliero-Universitaria di Cagliari. I risultati dell’Ospedale Sant’Orsola-Malpighi di Bologna erano stati precedentemente pubblicati. Gli aspetti tecnici della scialoendoscopia sono stati accuratamente descritti. I pazienti trattati presso l’Azienda Ospedaliero Universitaria di Cagliari presentavano una patologia unilaterale in 40 casi e bilaterale in 8 casi; sono state trattate 56 ghiandole salivari maggiori (22 sottomandibolari e 34 parotidi). 5 pazienti sono stati sottoposti a scialoendoscopia bilaterale per parotite ricorrente giovanile, 10 per patologia ostruttiva non litiasica e 33 (68,75%) presentavano calcoli salivari (1 paziente presentava una litiasi parotidea bilaterale). Solo 8 pazienti sono stati sottoposti a scialectomia radicale per via esterna (5 scialectomie sottomandibolare e 3 parotidectomie). La chirurgia conservativa nei pazienti con scialoadenite cronica ostruttiva appare efficace e può essere realizzata mediante un approccio puramente endoscopico o combinato, con un’alta percentuale di successo. La procedura richiede una strumentazione adeguata e deve essere eseguita da un chirurgo esperto, che abbia svolto un training specifico scialoendoscopico, in modo da evitare le possibili complicanze maggiori e minori. La scialectomia tradizionale rappresenta la “extrema ratio”, limitata nei casi in cui un approccio conservativo sia risultato inefficace o controindicato.
Keywords: Lithiasis; Obstructive sialadenitis; Salivary glands; Sialendoscopy.
© Copyright by Società Italiana di Otorinolaringologia e Chirurgia Cervico-Facciale, Rome, Italy.
Figures

References
-
- Bodner L. Salivary gland calculi: diagnostic imaging and surgical management. Compendium. 1993;14:572–572. 574-6, 578 passim. - PubMed
-
- Berini-Aytes L, Gay-Escoda C. Morbidity associated with removal of the submandibular gland. J Craniomaxillofac Surg. 1992;20:216–219. - PubMed
-
- Moeller K, Esser D, Boeger D, et al. Parotidectomy and submandibulectomy for benign diseases in Thuringia, Germany: a population-based study on epidemiology and outcome. Eur Arch Otorhinolaryngol. 2013;270:1149–1155. - PubMed
-
- McGurk M, Brown J. Alternatives for the treatment of salivary duct obstruction. Otolaryngol Clin North Am. 2009;42:1073–1085. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
