

Stockpiling Ventilators for Influenza Pandemics
- PMID: 28518041
- PMCID: PMC5443432
- DOI: 10.3201/eid2306.161417
Stockpiling Ventilators for Influenza Pandemics
Abstract
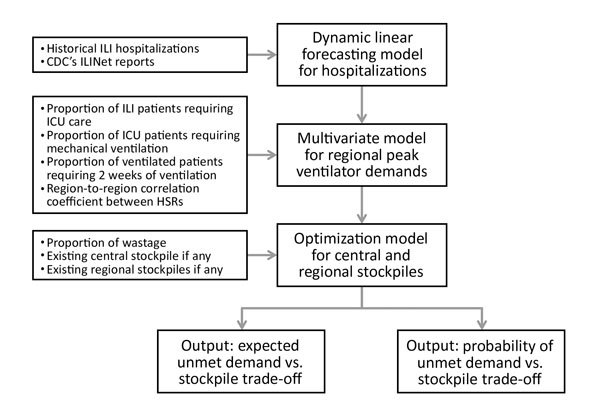
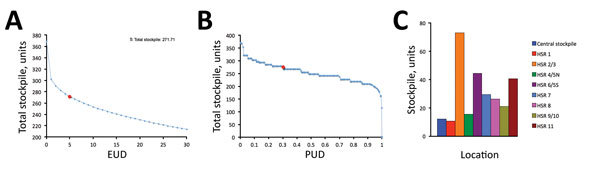
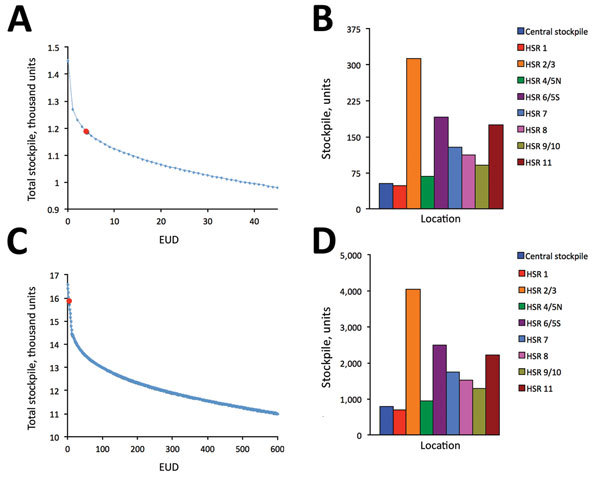
In preparing for influenza pandemics, public health agencies stockpile critical medical resources. Determining appropriate quantities and locations for such resources can be challenging, given the considerable uncertainty in the timing and severity of future pandemics. We introduce a method for optimizing stockpiles of mechanical ventilators, which are critical for treating hospitalized influenza patients in respiratory failure. As a case study, we consider the US state of Texas during mild, moderate, and severe pandemics. Optimal allocations prioritize local over central storage, even though the latter can be deployed adaptively, on the basis of real-time needs. This prioritization stems from high geographic correlations and the slightly lower treatment success assumed for centrally stockpiled ventilators. We developed our model and analysis in collaboration with academic researchers and a state public health agency and incorporated it into a Web-based decision-support tool for pandemic preparedness and response.
Keywords: Texas; United States; Ventilators; influenza; optimization; pandemic; viruses.
Figures
References
-
- US Department of Health and Human Services. Pandemic flu history. 2016. [cited 2016 Jun 16]. http://www.flu.gov/pandemic/history/index.html
-
- US Department of Health and Human Services. HHS pandemic influenza plan. 2005. [cited 2016 Jun 16]. http://www.flu.gov/planning-preparedness/federal/hhspandemicinfluenzapla...
-
- Sutton J, Tierney K. Disaster preparedness: concepts, guidance, and research. Fritz Institute Assessing Disaster Preparedness Conference; 2006 Nov 3–4; Sebastopol, CA, USA; 2006. [cited 2016 Jun 16]. http://www.fritzinstitute.org/pdfs/whitepaper/disasterpreparedness-conce...
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
