

Geographic variation and risk factors for systemic and limb ischemic events in patients with symptomatic peripheral artery disease: Insights from the REACH Registry
- PMID: 28520087
- PMCID: PMC6490387
- DOI: 10.1002/clc.22721
Geographic variation and risk factors for systemic and limb ischemic events in patients with symptomatic peripheral artery disease: Insights from the REACH Registry
Abstract
Background: Patients with symptomatic peripheral artery disease (PAD) are at high risk of ischemic events. However, data about predictors of this risk are limited.
Hypothesis: We analyzed baseline characteristics and 4-year follow-up of patients enrolled in the international REduction of Atherothrombosis for Continued Health (REACH) Registry with symptomatic PAD and no history of stroke/transient ischemic attack to describe annual rates of recurrent ischemic events globally and geographically.
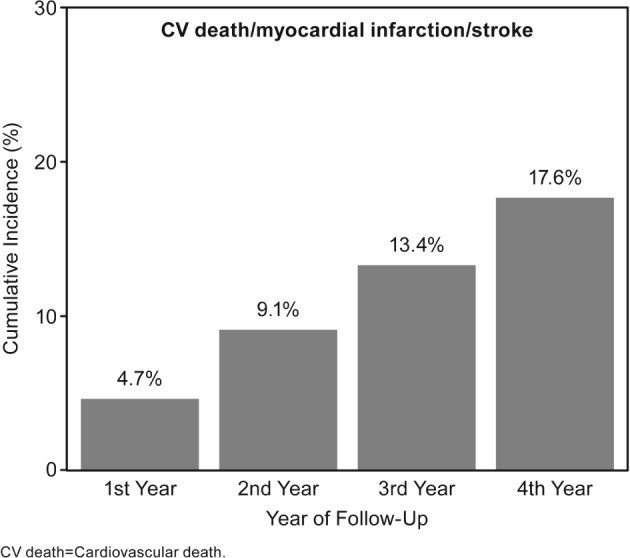
Methods: The primary outcome was systemic ischemic events (composite of cardiovascular death, myocardial infarction, or stroke) at 4 years. The secondary outcome was limb ischemic events (composite of lower limb amputation, peripheral bypass graft, and percutaneous intervention for PAD) at 2 years. Multivariate analysis identified risk factors associated with recurrent ischemic events.
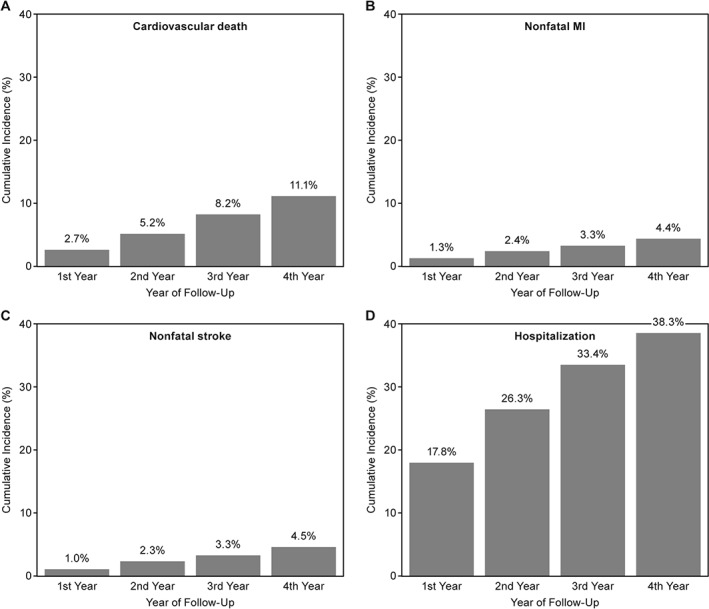
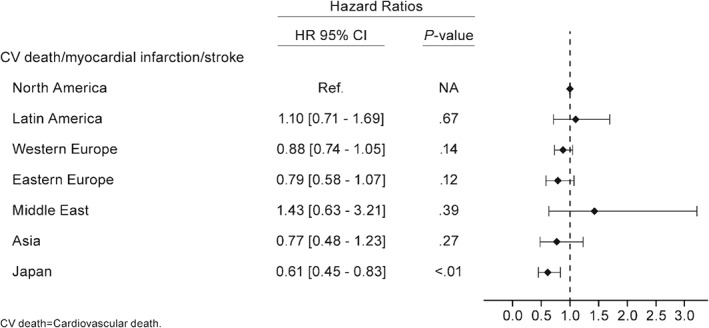
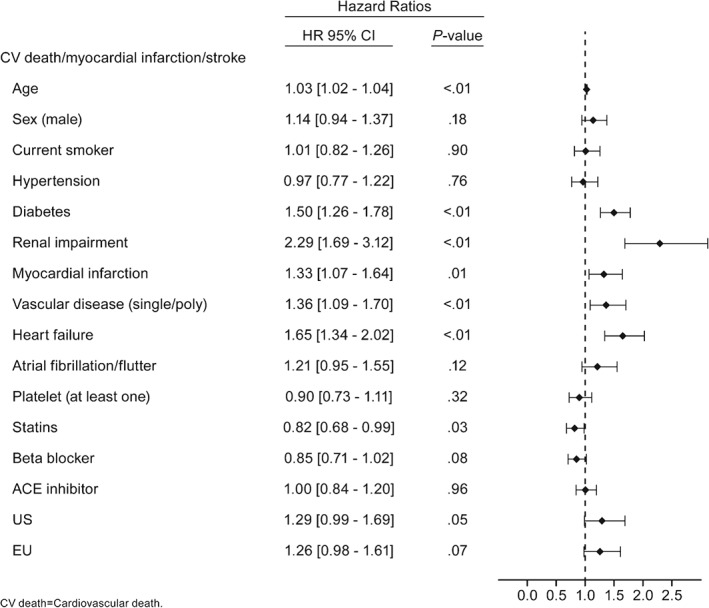
Results: The primary endpoint rate reached 4.7% during the first year and increased continuously (by 4%-5% each year) to 17.6% by year 4, driven mainly by cardiovascular mortality (11.1% at year 4). Japan experienced lower adjusted ischemic rates (P < 0.01) vs North America. Renal impairment (P < 0.01), congestive heart failure (P < 0.01), history of diabetes (P < 0.01), history of myocardial infarction (P = 0.01), vascular disease (single or poly, P < 0.01), and older age (P < 0.01) were associated with increased risk of systemic ischemic events, whereas statin use was associated with lower risk (P = 0.03). The limb ischemic event rate was 5.7% at 2 years.
Conclusions: Four-year systemic ischemic risk in patients with PAD and no history of stroke or transient ischemic attack remains high, and was mainly driven by cardiovascular mortality.
Keywords: Ischemic Risk; Peripheral Artery Disease; Vorapaxar.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
Dr. Deepak L. Bhatt discloses the following relationships: Advisory Board: Cardax, Elsevier Practice Update Cardiology, Medscape Cardiology, Regado Biosciences; Board of Directors: Boston VA Research Institute, Society of Cardiovascular Patient Care; Chair: American Heart Association Quality Oversight Committee; Data Monitoring Committees: Duke Clinical Research Institute, Harvard Clinical Research Institute, Mayo Clinic, Population Health Research Institute; Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News,
A full list of the REACH Registry investigators can be found in Bhatt DL, Steg PG, Ohman EM, et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis.
Figures
References
-
- Fowkes FG, Rudan D, Rudan I, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382:1329–1340. - PubMed
-
- Tendera M, Aboyans V, Bartelink ML, et al. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: the Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2011;32:2851–2906. - PubMed
-
- Violi F, Basili S, Berger JS, et al. Antiplatelet therapy in peripheral artery disease. Handb Exp Pharmacol. 2012;(210):547–563. - PubMed
-
- Criqui MH, Langer RD, Fronek A, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med. 1992;326:381–386. - PubMed
-
- Rothwell PM, Coull AJ, Silver LE, et al. Population‐based study of event‐rate, incidence, case fatality, and mortality for all acute vascular events in all arterial territories (Oxford Vascular Study). Lancet. 2005;366:1773–1783. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
