

Anger Self-Management Training for Chronic Moderate to Severe Traumatic Brain Injury: Results of a Randomized Controlled Trial
- PMID: 28520666
- PMCID: PMC5593756
- DOI: 10.1097/HTR.0000000000000316
Anger Self-Management Training for Chronic Moderate to Severe Traumatic Brain Injury: Results of a Randomized Controlled Trial
Abstract
Objective: To test efficacy of 8-session, 1:1 treatment, anger self-management training (ASMT), for chronic moderate to severe traumatic brain injury (TBI).
Setting: Three US outpatient treatment facilities.
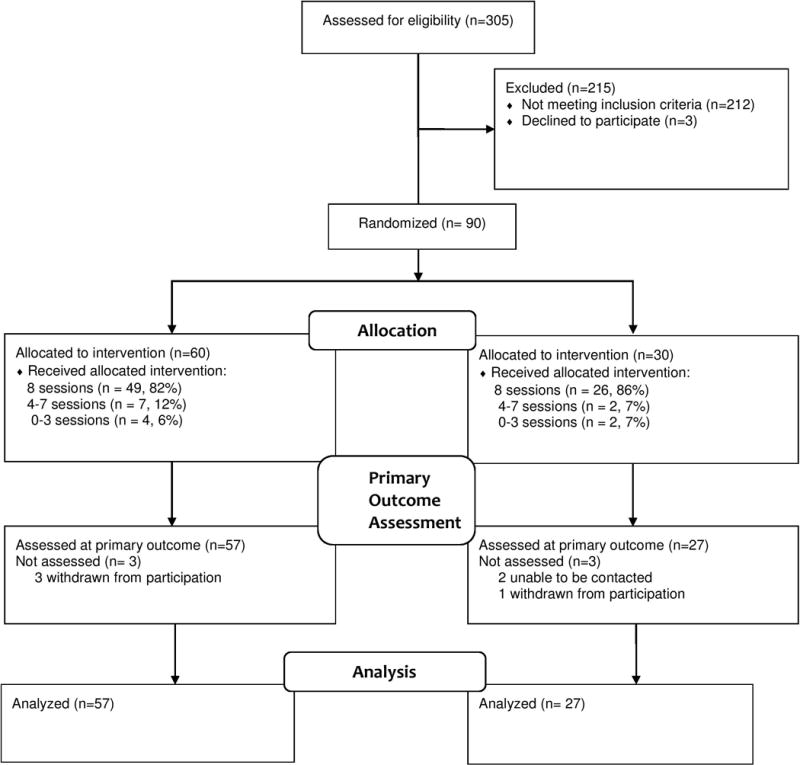
Participants: Ninety people with TBI and elevated self-reported anger; 76 significant others (SOs) provided collateral data.
Design: Multicenter randomized controlled trial with 2:1 randomization to ASMT or structurally equivalent comparison treatment, personal readjustment and education (PRE). Primary outcome assessment 1 week posttreatment; 8-week follow-up.
Primary outcome: Response to treatment defined as 1 or more standard deviation change in self-reported anger.
Secondary outcomes: SO-rated anger, emotional and behavioral status, satisfaction with life, timing of treatment response, participant and SO-rated global change, and treatment satisfaction.
Main measures: State-Trait Anger Expression Inventory-Revised Trait Anger (TA) and Anger Expression-Out (AX-O) subscales; Brief Anger-Aggression Questionnaire (BAAQ); Likert-type ratings of treatment satisfaction, global changes in anger and well-being.
Results: After treatment, ASMT response rate (68%) exceeded that of PRE (47%) on TA but not AX-O or BAAQ; this finding persisted at 8-week follow-up. No significant between-group differences in SO-reported response rates, emotional/behavioral status, or life satisfaction. ASMT participants were more satisfied with treatment and rated global change in anger as significantly better; SO ratings of global change in both anger and well-being were superior for ASMT.
Conclusion: ASMT was efficacious and persistent for some aspects of problematic anger. More research is needed to determine optimal dose and essential ingredients of behavioral treatment for anger after TBI.
Conflict of interest statement
Figures
Similar articles
-
Potential Impact of Amantadine on Aggression in Chronic Traumatic Brain Injury.J Head Trauma Rehabil. 2017 Sep/Oct;32(5):308-318. doi: 10.1097/HTR.0000000000000342. J Head Trauma Rehabil. 2017. PMID: 28891908 Clinical Trial.
-
Anger self-management training for people with traumatic brain injury: a preliminary investigation.J Head Trauma Rehabil. 2012 Mar-Apr;27(2):113-22. doi: 10.1097/HTR.0b013e31820e686c. J Head Trauma Rehabil. 2012. PMID: 21407088
-
Predictors of Treatment Response to a Psychoeducational Intervention for Anger in Chronic Moderate-Severe Traumatic Brain Injury.J Neuropsychiatry Clin Neurosci. 2023 Spring;35(2):158-164. doi: 10.1176/appi.neuropsych.21110279. Epub 2022 Aug 22. J Neuropsychiatry Clin Neurosci. 2023. PMID: 35989575 Clinical Trial.
-
Amantadine to Treat Cognitive Dysfunction in Moderate to Severe Traumatic Brain Injury.J Trauma Nurs. 2015 Jul-Aug;22(4):194-203; quiz E1-2. doi: 10.1097/JTN.0000000000000138. J Trauma Nurs. 2015. PMID: 26165872 Review.
-
Behavioral Clinical Trials in Moderate to Severe Pediatric Traumatic Brain Injury: Challenges, Potential Solutions, and Lessons Learned.J Head Trauma Rehabil. 2017 Nov/Dec;32(6):433-437. doi: 10.1097/HTR.0000000000000323. J Head Trauma Rehabil. 2017. PMID: 28520673 Free PMC article. Review.
Cited by
-
The Rehabilitation Treatment Specification System: Implications for Improvements in Research Design, Reporting, Replication, and Synthesis.Arch Phys Med Rehabil. 2019 Jan;100(1):146-155. doi: 10.1016/j.apmr.2018.09.112. Epub 2018 Sep 27. Arch Phys Med Rehabil. 2019. PMID: 30267666 Free PMC article.
-
Psychoeducational Interventions for Problematic Anger in Chronic Moderate to Severe Traumatic Brain Injury: A Study of Treatment Enactment.J Int Neuropsychol Soc. 2020 Jan;26(1):119-129. doi: 10.1017/S1355617719000833. J Int Neuropsychol Soc. 2020. PMID: 31983369 Free PMC article. Clinical Trial.
-
Delivery of Neuropsychological Interventions for Adult and Older Adult Clinical Populations: An Australian Expert Working Group Clinical Guidance Paper.Neuropsychol Rev. 2024 Dec;34(4):985-1047. doi: 10.1007/s11065-023-09624-0. Epub 2023 Nov 30. Neuropsychol Rev. 2024. PMID: 38032472 Free PMC article. Review.
-
Association between uncooperativeness and the glucose metabolism of patients with chronic behavioral disorders after severe traumatic brain injury: a cross-sectional retrospective study.Biopsychosoc Med. 2018 Apr 23;12:6. doi: 10.1186/s13030-018-0125-0. eCollection 2018. Biopsychosoc Med. 2018. PMID: 29713371 Free PMC article.
References
-
- Deb S, Lyons I, Koutzoukis C, Ali I, McCarthy G. Rate of psychiatric illness 1 year after traumatic brain injury. American Journal of Psychiatry. 1999;156(3):374–378. - PubMed
-
- Kim S, Manes F, Kosier T, Baruah S, Robinson R. Irritability following traumatic brain injury. Journal of Nervous and Mental Disease. 1999;187(6):327–335. - PubMed
-
- Bailie JM, Cole WR, Ivins B, et al. The experience, expression, and control of anger following traumatic brain injury in a military sample. The Journal of head trauma rehabilitation. 2015;30(1):12–20. - PubMed
-
- Hanks RA, Temkin N, Machamer J, Dikmen SS. Emotional and behavioral adjustment after traumatic brain injury. Archives of Physical Medicine and Rehabilitation. 1999;80(9):991–997. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
