

Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI
- PMID: 28521821
- PMCID: PMC5437672
- DOI: 10.1186/s13058-017-0846-1
Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI
Erratum in
-
Erratum to: Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI.Breast Cancer Res. 2017 Jul 10;19(1):80. doi: 10.1186/s13058-017-0862-1. Breast Cancer Res. 2017. PMID: 28693537 Free PMC article. No abstract available.
Abstract
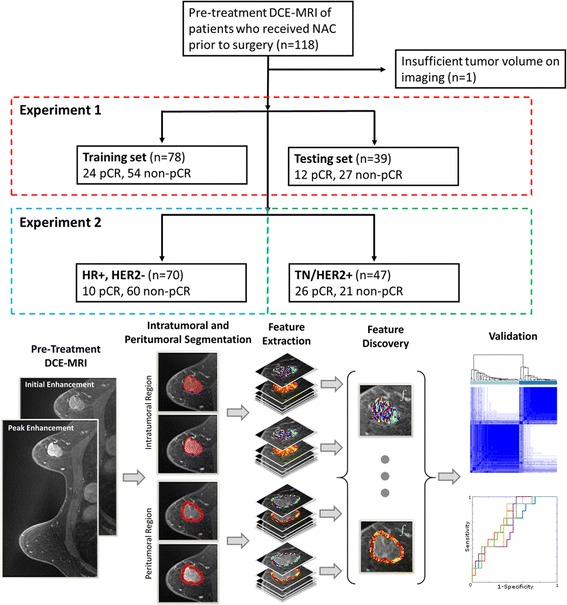
Background: In this study, we evaluated the ability of radiomic textural analysis of intratumoral and peritumoral regions on pretreatment breast cancer dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) to predict pathological complete response (pCR) to neoadjuvant chemotherapy (NAC).
Methods: A total of 117 patients who had received NAC were retrospectively analyzed. Within the intratumoral and peritumoral regions of T1-weighted contrast-enhanced MRI scans, a total of 99 radiomic textural features were computed at multiple phases. Feature selection was used to identify a set of top pCR-associated features from within a training set (n = 78), which were then used to train multiple machine learning classifiers to predict the likelihood of pCR for a given patient. Classifiers were then independently tested on 39 patients. Experiments were repeated separately among hormone receptor-positive and human epidermal growth factor receptor 2-negative (HR+, HER2-) and triple-negative or HER2+ (TN/HER2+) tumors via threefold cross-validation to determine whether receptor status-specific analysis could improve classification performance.
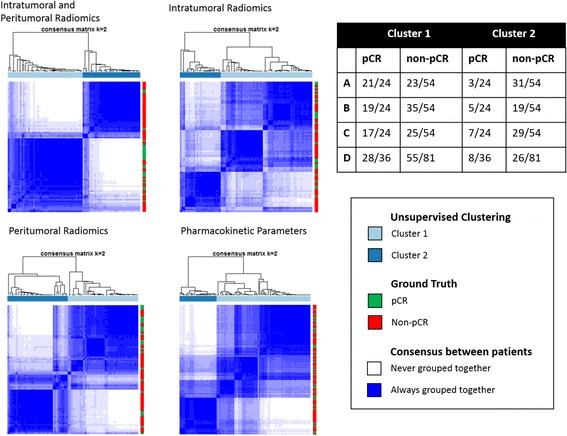
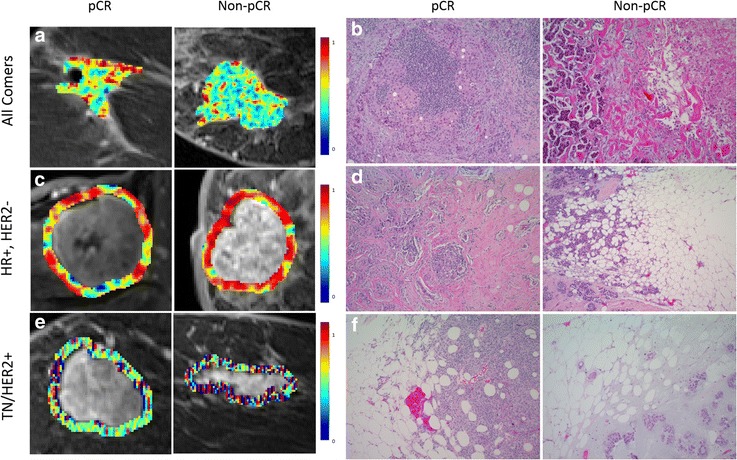
Results: Among all patients, a combined intratumoral and peritumoral radiomic feature set yielded a maximum AUC of 0.78 ± 0.030 within the training set and 0.74 within the independent testing set using a diagonal linear discriminant analysis (DLDA) classifier. Receptor status-specific feature discovery and classification enabled improved prediction of pCR, yielding maximum AUCs of 0.83 ± 0.025 within the HR+, HER2- group using DLDA and 0.93 ± 0.018 within the TN/HER2+ group using a naive Bayes classifier. In HR+, HER2- breast cancers, non-pCR was characterized by elevated peritumoral heterogeneity during initial contrast enhancement. However, TN/HER2+ tumors were best characterized by a speckled enhancement pattern within the peritumoral region of nonresponders. Radiomic features were found to strongly predict pCR independent of choice of classifier, suggesting their robustness as response predictors.
Conclusions: Through a combined intratumoral and peritumoral radiomics approach, we could successfully predict pCR to NAC from pretreatment breast DCE-MRI, both with and without a priori knowledge of receptor status. Further, our findings suggest that the radiomic features most predictive of response vary across different receptor subtypes.
Keywords: Imaging; MRI; Neoadjuvant chemotherapy; Personalized medicine; Radiomics; Treatment response.
Figures
Similar articles
-
Multivariate machine learning models for prediction of pathologic response to neoadjuvant therapy in breast cancer using MRI features: a study using an independent validation set.Breast Cancer Res Treat. 2019 Jan;173(2):455-463. doi: 10.1007/s10549-018-4990-9. Epub 2018 Oct 16. Breast Cancer Res Treat. 2019. PMID: 30328048 Free PMC article.
-
Predicting progression in triple-negative breast cancer patients undergoing neoadjuvant chemotherapy: Insights from peritumoral radiomics.Magn Reson Imaging. 2025 Feb;116:110292. doi: 10.1016/j.mri.2024.110292. Epub 2024 Dec 3. Magn Reson Imaging. 2025. PMID: 39631160
-
Development and validation of peritumoral vascular and intratumoral radiomics to predict pathologic complete responses to neoadjuvant chemotherapy in patients with triple-negative breast cancer.BMC Med Imaging. 2024 Jun 6;24(1):136. doi: 10.1186/s12880-024-01311-7. BMC Med Imaging. 2024. PMID: 38844842 Free PMC article.
-
Complete pathologic response rate to neoadjuvant chemotherapy increases with increasing HER2/CEP17 ratio in HER2 overexpressing breast cancer: analysis of the National Cancer Database (NCDB).Breast Cancer Res Treat. 2020 Jun;181(2):249-254. doi: 10.1007/s10549-020-05599-1. Epub 2020 Apr 10. Breast Cancer Res Treat. 2020. PMID: 32277375 Review.
-
Tumor necrosis by pretreatment breast MRI: association with neoadjuvant systemic therapy (NAST) response in triple-negative breast cancer (TNBC).Breast Cancer Res Treat. 2021 Jan;185(1):1-12. doi: 10.1007/s10549-020-05917-7. Epub 2020 Sep 13. Breast Cancer Res Treat. 2021. PMID: 32920733 Free PMC article. Review.
Cited by
-
Predicting the Level of Tumor-Infiltrating Lymphocytes in Patients With Breast Cancer: Usefulness of Mammographic Radiomics Features.Front Oncol. 2021 Mar 11;11:628577. doi: 10.3389/fonc.2021.628577. eCollection 2021. Front Oncol. 2021. PMID: 33777776 Free PMC article.
-
Magnetic resonance radiomics signatures for predicting poorly differentiated hepatocellular carcinoma: A SQUIRE-compliant study.Medicine (Baltimore). 2021 May 14;100(19):e25838. doi: 10.1097/MD.0000000000025838. Medicine (Baltimore). 2021. PMID: 34106622 Free PMC article.
-
Texture-Based Radiomic SD-OCT Features Associated With Response to Anti-VEGF Therapy in a Phase III Neovascular AMD Clinical Trial.Transl Vis Sci Technol. 2024 Jan 2;13(1):29. doi: 10.1167/tvst.13.1.29. Transl Vis Sci Technol. 2024. PMID: 38289610 Free PMC article. Clinical Trial.
-
Application of Radiomics and Decision Support Systems for Breast MR Differential Diagnosis.Comput Math Methods Med. 2018 Sep 23;2018:7417126. doi: 10.1155/2018/7417126. eCollection 2018. Comput Math Methods Med. 2018. PMID: 30344618 Free PMC article. Review.
-
Impact of Machine Learning With Multiparametric Magnetic Resonance Imaging of the Breast for Early Prediction of Response to Neoadjuvant Chemotherapy and Survival Outcomes in Breast Cancer Patients.Invest Radiol. 2019 Feb;54(2):110-117. doi: 10.1097/RLI.0000000000000518. Invest Radiol. 2019. PMID: 30358693 Free PMC article.
References
-
- American Cancer Society. Breast cancer facts & figures. http://www.cancer.org/research/cancerfactsstatistics/breast-cancer-facts.... Accessed 8 Dec 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
