

Systolic Blood Pressure Within 24 Hours After Thrombectomy for Acute Ischemic Stroke Correlates With Outcome
- PMID: 28522673
- PMCID: PMC5524120
- DOI: 10.1161/JAHA.117.006167
Systolic Blood Pressure Within 24 Hours After Thrombectomy for Acute Ischemic Stroke Correlates With Outcome
Abstract
Background: Current guidelines suggest treating blood pressure above 180/105 mm Hg during the first 24 hours in patients with acute ischemic stroke undergoing any form of recanalization therapy. Currently, no studies exist to guide blood pressure management in patients with stroke treated specifically with mechanical thrombectomy. We aimed to determine the association between blood pressure parameters within the first 24 hours after mechanical thrombectomy and patient outcomes.
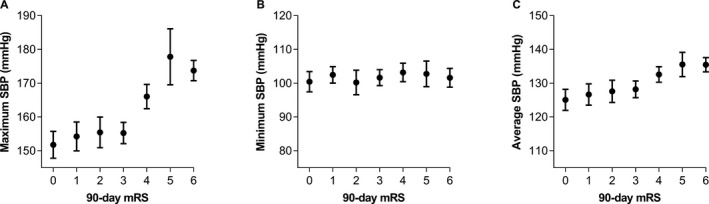
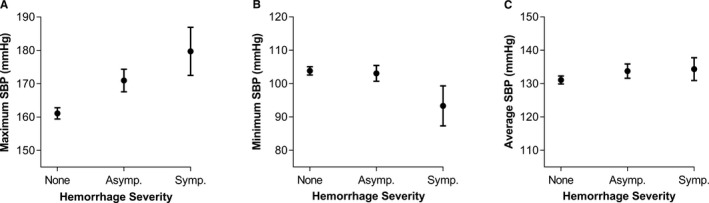
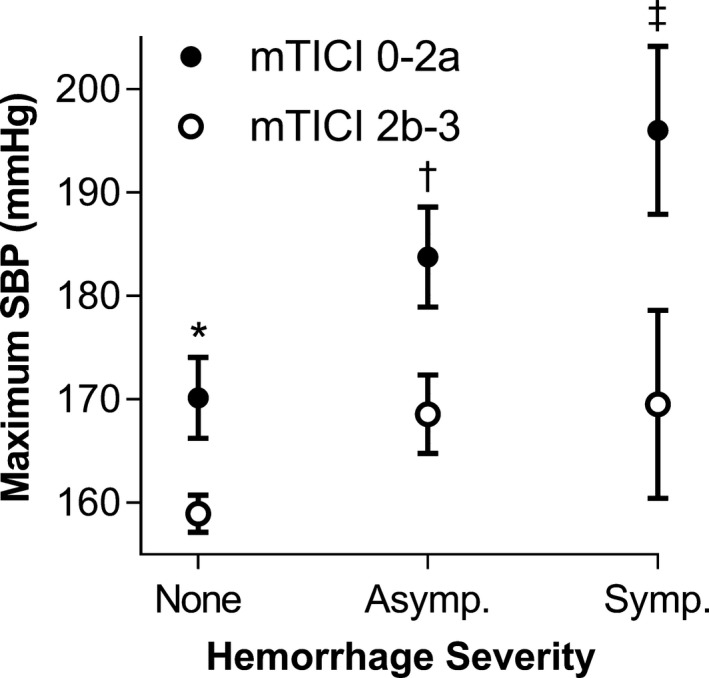
Methods and results: We retrospectively studied a consecutive sample of adult patients who underwent mechanical thrombectomy for acute ischemic stroke of the anterior cerebral circulation at 3 institutions from March 2015 to October 2016. We collected the values of maximum, minimum, and average values of systolic blood pressure, diastolic blood pressure, and mean arterial pressures in the first 24 hours after mechanical thrombectomy. Primary and secondary outcomes were patients' functional status at 90 days measured on the modified Rankin scale and the incidence and severity of intracranial hemorrhages within 48 hours. Associations were explored using an ordered multivariable logistic regression analyses. A total of 228 patients were included (mean age 65.8±14.3; 104 males, 45.6%). Maximum systolic blood pressure independently correlated with a worse 90-day modified Rankin scale and hemorrhagic complications within 48 hours (adjusted odds ratio=1.02 [1.01-1.03], P=0.004; 1.02 [1.01-1.04], P=0.002; respectively) in multivariable analyses, after adjusting for several possible confounders.
Conclusions: Higher peak values of systolic blood pressure independently correlated with worse 90-day modified Rankin scale and a higher rate of hemorrhagic complications. Further prospective studies are warranted to identify whether systolic blood pressure is a therapeutic target to improve outcomes.
Keywords: blood pressure; hemorrhage; outcome; stroke; thrombectomy.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, Albers GW, Cognard C, Cohen DJ, Hacke W, Jansen O, Jovin TG, Mattle HP, Nogueira RG, Siddiqui AH, Yavagal DR, Baxter BW, Devlin TG, Lopes DK, Reddy VK, du Mesnil de Rochemont R, Singer OC, Jahan R; Investigators SP . Stent‐retriever thrombectomy after intravenous t‐PA vs. t‐PA alone in stroke. N Engl J Med. 2015;372:2285–2295. - PubMed
-
- Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, San Roman L, Serena J, Abilleira S, Ribo M, Millan M, Urra X, Cardona P, Lopez‐Cancio E, Tomasello A, Castano C, Blasco J, Aja L, Dorado L, Quesada H, Rubiera M, Hernandez‐Perez M, Goyal M, Demchuk AM, von Kummer R, Gallofre M, Davalos A; Investigators RT . Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 2015;372:2296–2306. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, Roy D, Jovin TG, Willinsky RA, Sapkota BL, Dowlatshahi D, Frei DF, Kamal NR, Montanera WJ, Poppe AY, Ryckborst KJ, Silver FL, Shuaib A, Tampieri D, Williams D, Bang OY, Baxter BW, Burns PA, Choe H, Heo JH, Holmstedt CA, Jankowitz B, Kelly M, Linares G, Mandzia JL, Shankar J, Sohn SI, Swartz RH, Barber PA, Coutts SB, Smith EE, Morrish WF, Weill A, Subramaniam S, Mitha AP, Wong JH, Lowerison MW, Sajobi TT, Hill MD; Investigators ET . Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372:1019–1030. - PubMed
-
- Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, Yan B, Dowling RJ, Parsons MW, Oxley TJ, Wu TY, Brooks M, Simpson MA, Miteff F, Levi CR, Krause M, Harrington TJ, Faulder KC, Steinfort BS, Priglinger M, Ang T, Scroop R, Barber PA, McGuinness B, Wijeratne T, Phan TG, Chong W, Chandra RV, Bladin CF, Badve M, Rice H, de Villiers L, Ma H, Desmond PM, Donnan GA, Davis SM; Investigators E‐I . Endovascular therapy for ischemic stroke with perfusion‐imaging selection. N Engl J Med. 2015;372:1009–1018. - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, Schonewille WJ, Vos JA, Nederkoorn PJ, Wermer MJ, van Walderveen MA, Staals J, Hofmeijer J, van Oostayen JA, Lycklama a Nijeholt GJ, Boiten J, Brouwer PA, Emmer BJ, de Bruijn SF, van Dijk LC, Kappelle LJ, Lo RH, van Dijk EJ, de Vries J, de Kort PL, van Rooij WJ, van den Berg JS, van Hasselt BA, Aerden LA, Dallinga RJ, Visser MC, Bot JC, Vroomen PC, Eshghi O, Schreuder TH, Heijboer RJ, Keizer K, Tielbeek AV, den Hertog HM, Gerrits DG, van den Berg‐Vos RM, Karas GB, Steyerberg EW, Flach HZ, Marquering HA, Sprengers ME, Jenniskens SF, Beenen LF, van den Berg R, Koudstaal PJ, van Zwam WH, Roos YB, van der Lugt A, van Oostenbrugge RJ, Majoie CB, Dippel DW; Investigators MC . A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
