

Effects of Sodium-Glucose Cotransporter 2 Inhibitors on 24-Hour Ambulatory Blood Pressure: A Systematic Review and Meta-Analysis
- PMID: 28522675
- PMCID: PMC5524106
- DOI: 10.1161/JAHA.117.005686
Effects of Sodium-Glucose Cotransporter 2 Inhibitors on 24-Hour Ambulatory Blood Pressure: A Systematic Review and Meta-Analysis
Abstract
Background: Sodium-glucose cotransporter 2 (SGLT2) inhibitors are a novel class of antihyperglycemic agents that improve glycemic control by increasing glycosuria. Additional benefits beyond glucose lowering include significant improvements in seated clinic blood pressure (BP), partly attributed to their diuretic-like actions. Less known are the effects of this class on 24-hour ambulatory BP, which is a better predictor of cardiovascular risk than seated clinic BP.
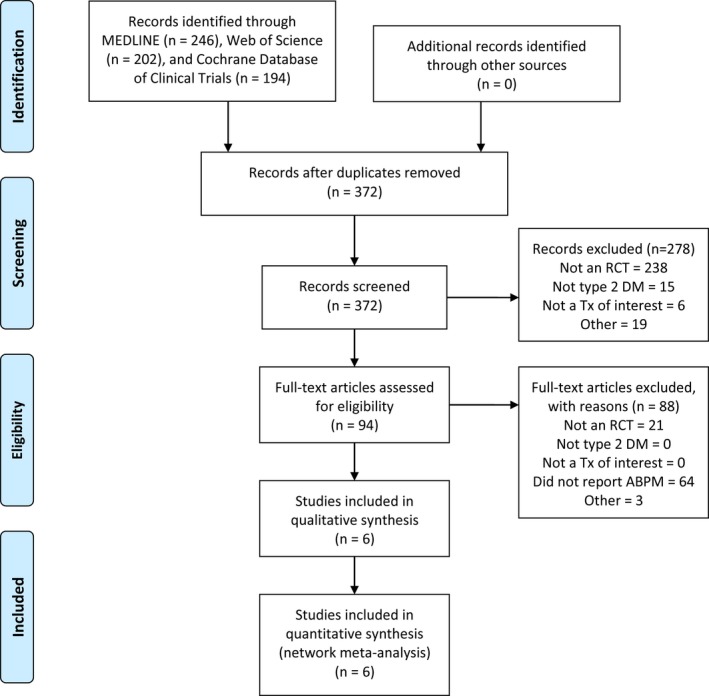
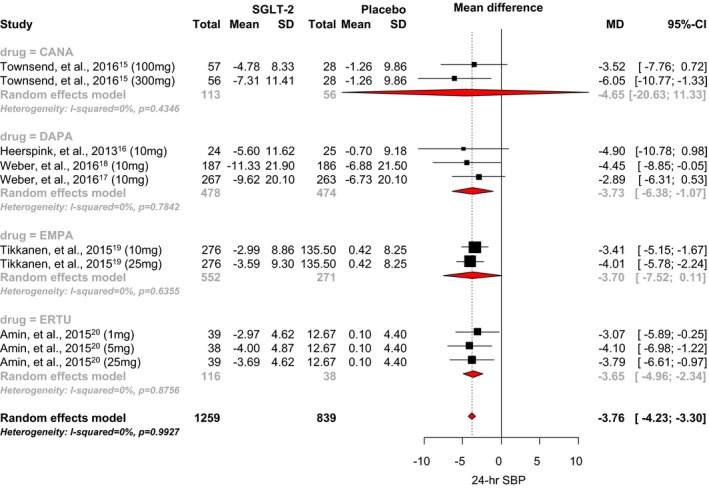
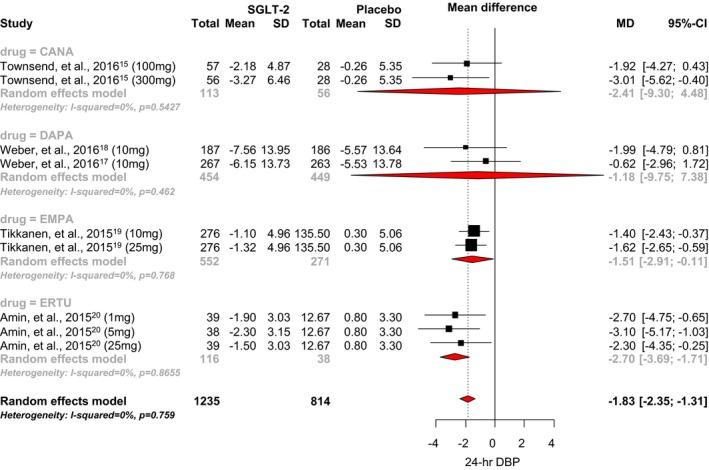
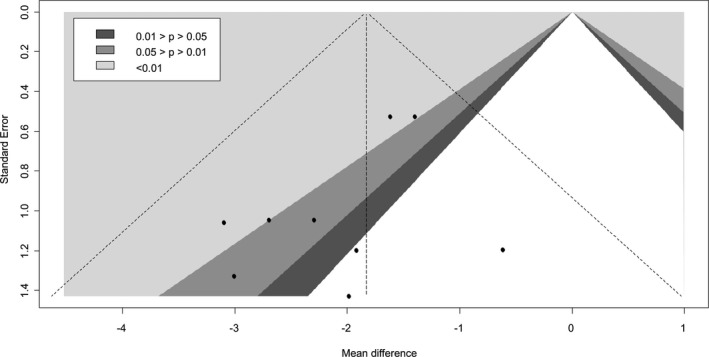
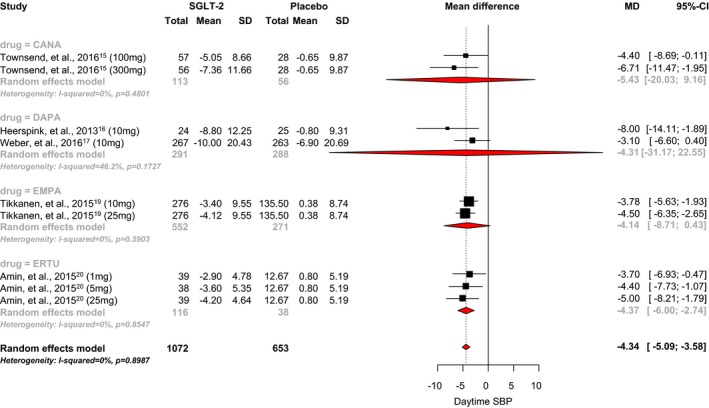
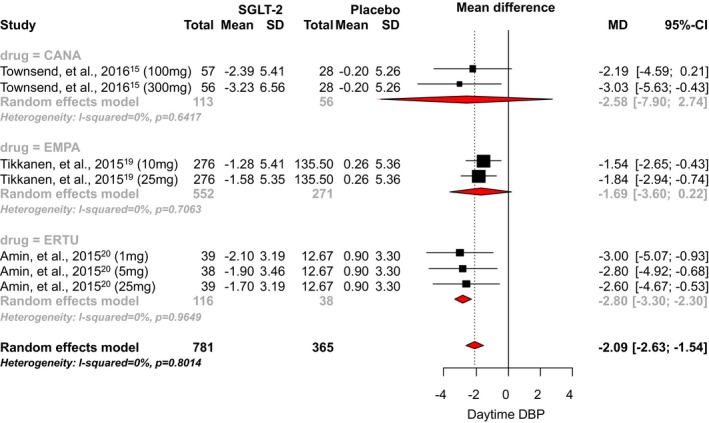
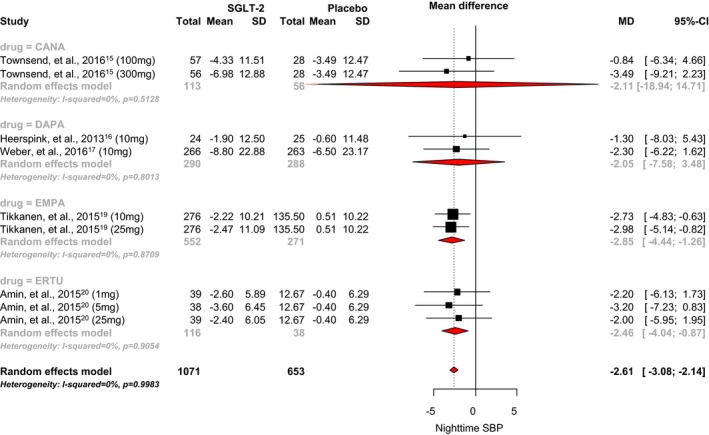
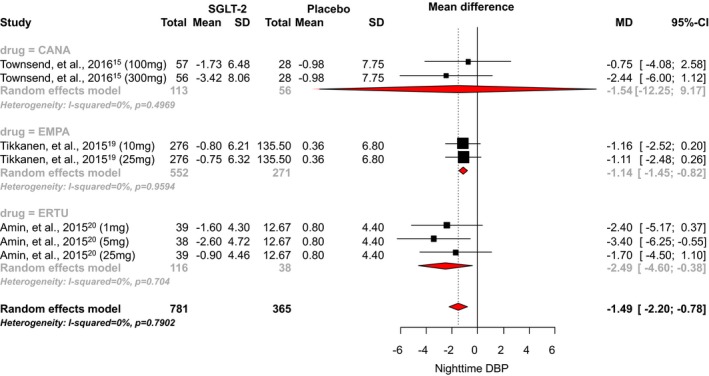
Methods and results: We performed a meta-analysis of randomized, double-blind, placebo-controlled trials to investigate the effects of SGLT2 inhibitors on 24-hour ambulatory BP. We searched all studies published before August 17, 2016, which reported 24-hour ambulatory BP data. Mean differences in 24-hour BP, daytime BP, and nighttime BP were calculated by a random-effects model. SGLT2 inhibitors significantly reduce 24-hour ambulatory systolic and diastolic BP by -3.76 mm Hg (95% CI, -4.23 to -2.34; I2=0.99) and -1.83 mm Hg (95% CI, -2.35 to -1.31; I2=0.76), respectively. Significant reductions in daytime and nighttime systolic and diastolic BP were also found. No association between baseline BP or change in body weight were observed.
Conclusions: This meta-analysis shows that the reduction in 24-hour ambulatory BP observed with SGLT2 inhibitors is a class effect. The diurnal effect of SGLT2 inhibitors on 24-hour ambulatory BP may contribute to their favorable effects on cardiovascular outcomes.
Keywords: ambulatory blood pressure monitoring; diabetes mellitus; diabetic therapy/glitazones; high blood pressure; hypertension; metformin; sodium‐glucose cotransporter 2 inhibitors.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- DeFronzo RA, Norton L, Abdul‐Ghani M. Renal, metabolic and cardiovascular considerations of SGLT2 inhibition. Nat Rev Nephrol. 2016;13:11–26. - PubMed
-
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedi JC, Inzucchi SE. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–2128. - PubMed
-
- U.S. Food and Drug Administration . FDA approves Jardiance to reduce cardiovascular death in adults with type 2 diabetes. Available at: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm531517.htm. Accessed January 11, 2017.
-
- Baker WL, Smyth LR, Riche DM, Bourret EM, Chamberlin KW, White WB. Effects of sodium‐glucose co‐transporter 2 inhibitors on blood pressure: a systematic review and meta‐analysis. J Am Soc Hypertens. 2014;8:262–275. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
