

Efficacy of anti-PD-1 therapy in patients with melanoma brain metastases
- PMID: 28524161
- PMCID: PMC5518864
- DOI: 10.1038/bjc.2017.142
Efficacy of anti-PD-1 therapy in patients with melanoma brain metastases
Abstract
Background: There is limited data on the efficacy of anti-programmed death 1 (PD-1) antibodies in patients (pts) with melanoma brain metastasis (BM), particularly those which are symptomatic.
Method: We retrospectively assessed pts with melanoma BM treated with PD-1 antibodies, nivolumab and pembrolizumab. Clinicopathologic and treatment parameters were collected and outcomes determined for intracranial (IC) response rate (RR) using a modified RECIST criteria, with up to five IC target lesions used to determine IC response, disease control rate (DCR) and progression-free survival (PFS).
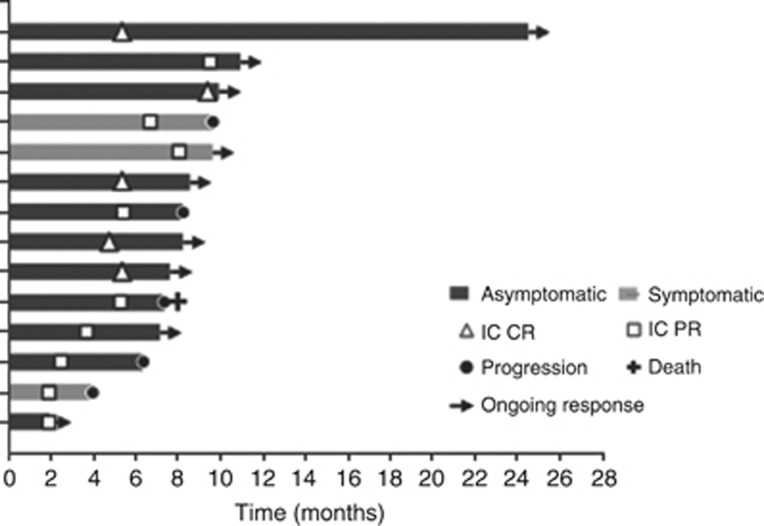
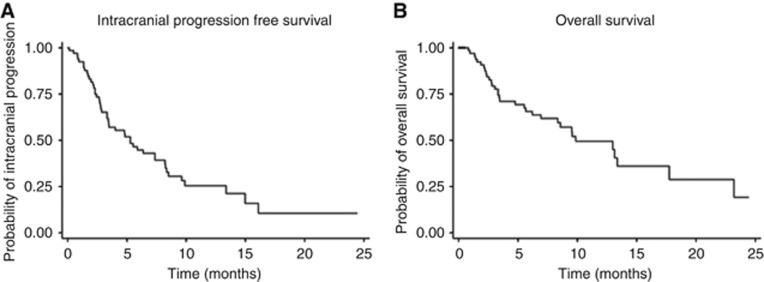
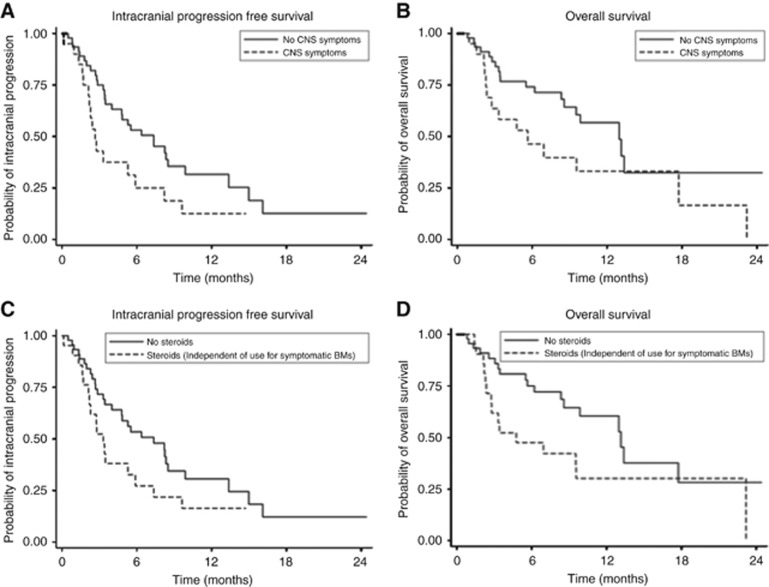
Results: A total of 66 pts were identified with a median follow up of 7.0 months (range 0.8-24.5 months). A total of 68% were male and 45% BRAF V600 mutation positive. At PD-1 antibody commencement, 50% had an elevated LDH; 64% had local therapy to BM prior to commencing anti-PD1, of which 5% had surgical resection, 14% stereotactic radiosurgery (SRS), 18% whole-brain radiotherapy (WBRT), 27% had surgery and radiotherapy. Twenty-one per cent started anti-PD-1 as first line systemic therapy. No pt had prior anti-PD-1 treatment. The IC overall RR was 21 and DCR 56%. Responses occurred in 21% of pts with symptomatic BM. The median OS was 9.9 months (95% CI 6.93-17.74). Pts with symptomatic BM had shorter PFS than those without symptoms (2.7 vs 7.4 months, P=0.035) and numerically shorter OS (5.7 vs 13.0 months, P=0.068). Pts requiring corticosteroids also had a numerically shorter PFS (3.2 vs 7.4 months, P=0.081) and OS (4.8 vs 13.1 months, P=0.039).
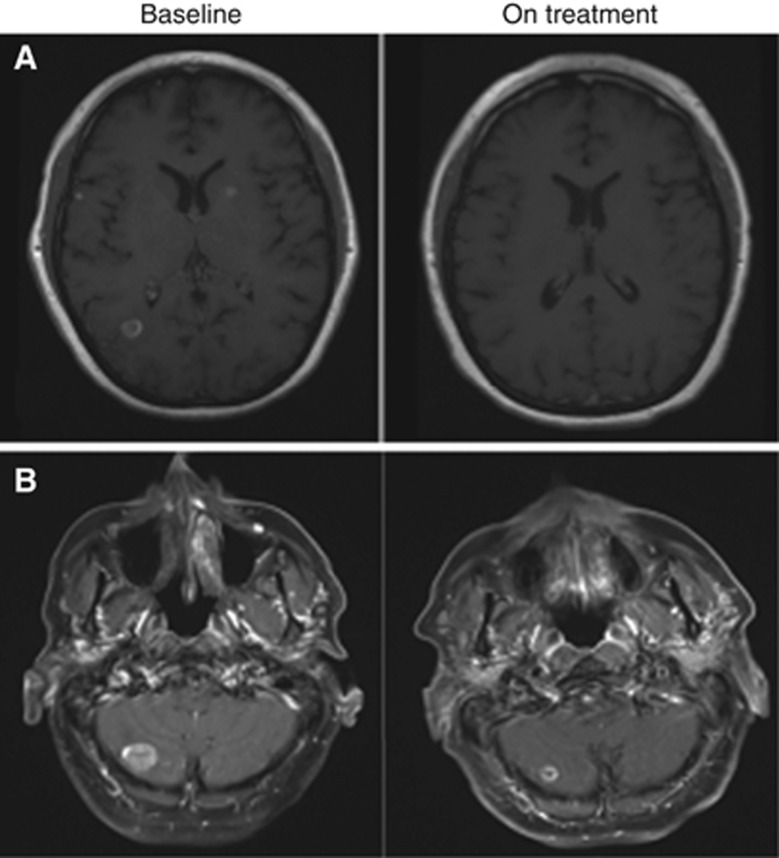
Conclusions: IC responses to anti-PD-1 antibodies occur in pts with BM, including those with symptomatic BM requiring corticosteroids. Prospective trials evaluating anti-PD-1 therapy in pts with BM are underway.
Conflict of interest statement
JC has sat on advisory boards for Novartis and GSK; RFK is a consultant advisor for Merck, BMS, Novartis and Amgen; GVL is a consultant advisor to Amgen, Merck MSD, Novartis, Roche, Array and Pierre-Fabre; AMM is a consultant advisor to Merck MSD, Norvatis and Chugai; MSC is a consultant advisor for Merck MSD, BMS, Novartis and Amgen. The remaining authors declare no conflict of interest.
Figures
References
-
- Ahmed K, Abuodeh Y, Echevarria M, Arrington J, Stallworth D, Hogue C, Naghavi A, Kim S, Kim Y, Patel B, Sarangkasiri S, Johnstone PA, Sahebjam S, Khushalani N, Forsyth PA, Harrison LB, Yu M, Etame AB, Caudell JJ (2016) Clinical outcomes of melanoma brain metastases treated with stereotactic radiosurgery and anti-PD-1 therapy, anti-CTLA-4 therapy, BRAF/MEK inhibitors, BRAF inhibitor, or conventional chemotherapy. Ann Oncol 27(12): 2288–2294. - PMC - PubMed
-
- Ahmed K, Stallworth D, Kim Y, Johnstone P, Harrison L, Caudell J, Yu H, Etame A, Weber J, Gibney G (2015) Clinical outcomes of melanoma brain metastases treated with stereotactic radiation and anti-PD-1 therapy. Ann Oncol 27(3): 434–441. - PubMed
-
- Azer MW, Menzies AM, Haydu LE, Kefford RF, Long GV (2014) Patterns of response and progression in patients with BRAF-mutant melanoma metastatic to the brain who were treated with dabrafenib. Cancer 120: 530–536. - PubMed
-
- Carlino MS, Fogarty GB, Long GV (2012) Treatment of melanoma brain metastases: a new paradigm. Cancer J 18: 208–212. - PubMed
-
- Choong ES, Lo S, Drummond M, Fogarty GB, Menzies AM, Guminski A, Shivalingam B, Clarke K, Long GV, Hong AM (2017) Survival of patients with melanoma brain metastasis treated with stereotactic radiosurgery and active systemic drug therapies. Eur J Cancer 75: 169–178. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
