

Biological and clinical evidence for somatic mutations in BRCA1 and BRCA2 as predictive markers for olaparib response in high-grade serous ovarian cancers in the maintenance setting
- PMID: 28525389
- PMCID: PMC5546431
- DOI: 10.18632/oncotarget.17613
Biological and clinical evidence for somatic mutations in BRCA1 and BRCA2 as predictive markers for olaparib response in high-grade serous ovarian cancers in the maintenance setting
Abstract
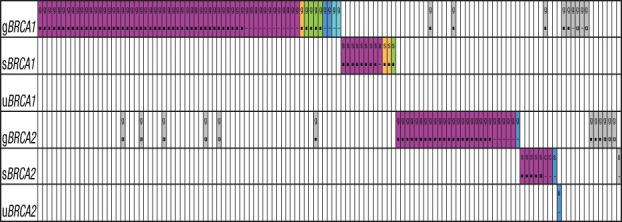
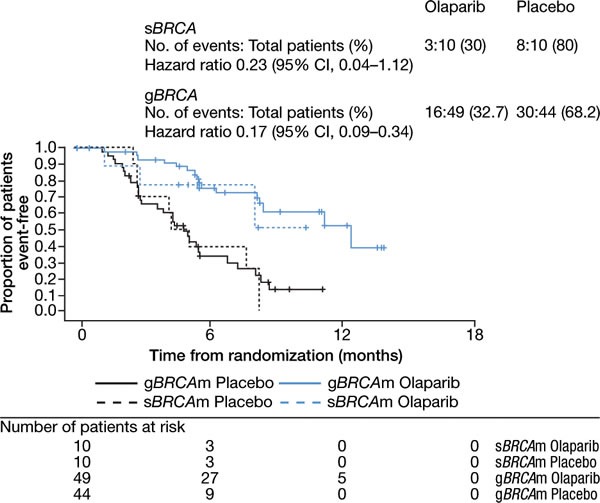
To gain a better understanding of the role of somatic mutations in olaparib response, next-generation sequencing (NGS) of BRCA1 and BRCA2 was performed as part of a planned retrospective analysis of tumors from a randomized, double-blind, Phase II trial (Study 19; D0810C00019; NCT00753545) in 265 patients with platinum-sensitive high-grade serous ovarian cancer. BRCA1/2 loss-of-function mutations were found in 55% (114/209) of tumors, were mutually exclusive, and demonstrated high concordance with Sanger-sequenced germline mutations in matched blood samples, confirming the accuracy (97%) of tumor BRCA1/2 NGS testing. Additionally, NGS identified somatic mutations absent from germline testing in 10% (20/209) of the patients. Somatic mutations had >80% biallelic inactivation frequency and were predominantly clonal, suggesting that BRCA1/2 loss occurs early in the development of these cancers. Clinical outcomes between placebo- and olaparib-treated patients with somatic BRCA1/2 mutations were similar to those with germline BRCA1/2 mutations, indicating that patients with somatic BRCA1/2 mutations benefit from treatment with olaparib.
Keywords: BRCA; germline; olaparib; ovarian; somatic.
Conflict of interest statement
B.A.D., Z.L, D.R.H., M.C.M.O., S.K.S., J.D.R., T.W.H., and J.C.B are employees of and shareholders in AstraZeneca. M.H., J.S., and R.Y. are employees of and shareholders in Foundation Medicine. J.A.L. is a principal investigator of Study 19 and has received funding from AstraZeneca to attend advisory boards and to give lectures.
Figures
References
-
- Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, Lopez E, Kyle S, Meuth M, Curtin NJ, Helleday T. Specific killing of BRCA2-deficient tumours with inhibitors of poly(ADP-ribose) polymerase. Nature. 2005;434:913–917. - PubMed
-
- Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB, Santarosa M, Dillon KJ, Hickson I, Knights C, Martin NM, Jackson SP, Smith GC, et al. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature. 2005;434:917–921. - PubMed
-
- Hall JM, Lee MK, Newman B, Morrow JE, Anderson LA, Huey B, King MC. Linkage of early-onset familial breast cancer to chromosome 17q21. Science. 1990;250:1684–1689. - PubMed
-
- Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavtigian S, Liu Q, Cochran C, Bennett LM, Ding W, Bell R, Rosenthal J, Husse C, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994;266:66–71. - PubMed
-
- Futreal PA, Liu Q, Shattuck-Eidens D, Cochran C, Harshman K, Tavtigian S, Bennett LM, Haugen-Strano A, Swensen J, Miki Y, Eddington K, McClure M, Frye C, et al. BRCA1 mutations in primary breast and ovarian carcinomas. Science. 1994;266:120–122. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
