

Hemoadsorption treatment of patients with acute infective endocarditis during surgery with cardiopulmonary bypass - a case series
- PMID: 28525670
- PMCID: PMC6159853
- DOI: 10.5301/ijao.5000583
Hemoadsorption treatment of patients with acute infective endocarditis during surgery with cardiopulmonary bypass - a case series
Abstract
Introduction: Infective endocarditis is a serious disease condition. Depending on the causative microorganism and clinical symptoms, cardiac surgery and valve replacement may be needed, posing additional risks to patients who may simultaneously suffer from septic shock. The combination of surgery bacterial spreadout and artificial cardiopulmonary bypass (CPB) surfaces results in a release of key inflammatory mediators leading to an overshooting systemic hyperinflammatory state frequently associated with compromised hemodynamic and organ function. Hemoadsorption might represent a potential approach to control the hyperinflammatory systemic reaction associated with the procedure itself and subsequent clinical conditions by reducing a broad range of immuno-regulatory mediators.
Methods: We describe 39 cardiac surgery patients with proven acute infective endocarditis obtaining valve replacement during CPB surgery in combination with intraoperative CytoSorb hemoadsorption. In comparison, we evaluated a historical group of 28 patients with infective endocarditis undergoing CPB surgery without intraoperative hemoadsorption.
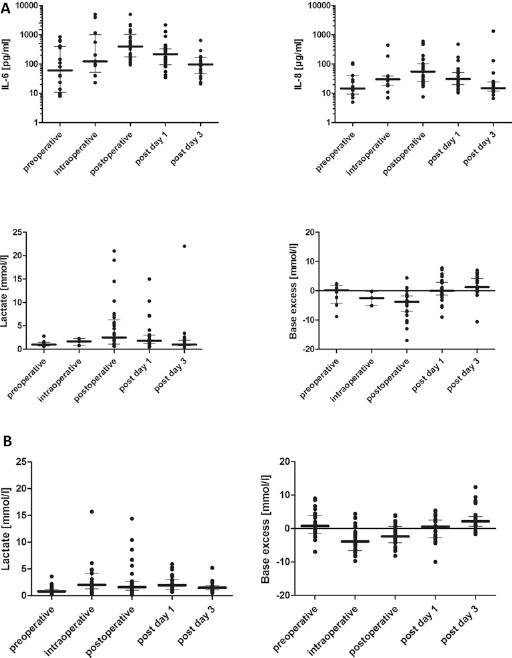
Results: CytoSorb treatment was associated with a mitigated postoperative response of key cytokines and clinical metabolic parameters. Moreover, patients showed hemodynamic stability during and after the operation while the need for vasopressors was less pronounced within hours after completion of the procedure, which possibly could be attributed to the additional CytoSorb treatment. Intraoperative hemoperfusion treatment was well tolerated and safe without the occurrence of any CytoSorb device-related adverse event.
Conclusions: Thus, this interventional approach may open up potentially promising therapeutic options for critically-ill patients with acute infective endocarditis during and after cardiac surgery, with cytokine reduction, improved hemodynamic stability and organ function as seen in our patients.
Conflict of interest statement
Conflict of interest: KT and GF received honoraria for lectures from Cytosorbents. KT has an advisory contract with Cytosorbents. The other authors have no conflicts of interest associated with this report.
Figures

References
-
- Carrel T., Englberger L., Takala J.. Whats new in surgical treatment of infective endocarditis? Intensive Care Med. 2016; 42(12): 2052–2054. - PubMed
-
- The 2015 ESC Guidelines for the management of infective endocarditis. Eur Heart J. 2015; 36(44): 3036–3037. - PubMed
-
- Cremer J., Martin M., Redl H. et al. Systemic inflammatory response syndrome after cardiac operations. Ann Thorac Surg. 1996; 61(6): 1714–1720. - PubMed
-
- Born F., Pichlmaier M., Peterß S. et al. Systemic Inflammatory Response Syndrome in in Heart Surgery: New possibilities for treatment through the use of a cytokine adsorber during ECC? Kardiotechnik. 2014; 2: 1–10 http://armaghansalamat.com/media/brands/Cytosorbents/Literature/2014_Bor.... Accessed April 24, 2017.
-
- Träger K., Fritzler D., Fischer G. et al. Treatment of post-cardiopulmonary bypass SIRS by hemoadsorption: a case series. Int J Artif Organs. 2016; 39(3): 141–146. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
