

The optimal extent of gastrectomy for middle-third gastric cancer: distal subtotal gastrectomy is superior to total gastrectomy in short-term effect without sacrificing long-term survival
- PMID: 28526077
- PMCID: PMC5437661
- DOI: 10.1186/s12885-017-3343-0
The optimal extent of gastrectomy for middle-third gastric cancer: distal subtotal gastrectomy is superior to total gastrectomy in short-term effect without sacrificing long-term survival
Abstract
Background: The optimal extent of gastrectomy for middle-third gastric cancer remains controversial. In our study, the short-term effects and longer-term survival outcomes of distal subtotal gastrectomy and total gastrectomy are analysed to determine the optimal extent of gastrectomy for middle-third gastric cancer.
Methods: We retrospectively collect and analyse clinicopathologic data and follow-up outcomes from a prospectively collected database at the Peking University Cancer Hospital. Patients with middle-third gastric adenocarcinoma who underwent curative resection are enrolled in our study.
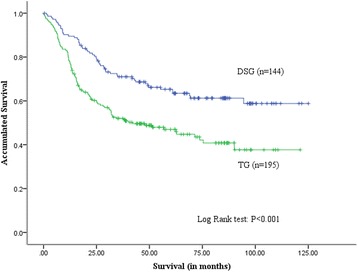
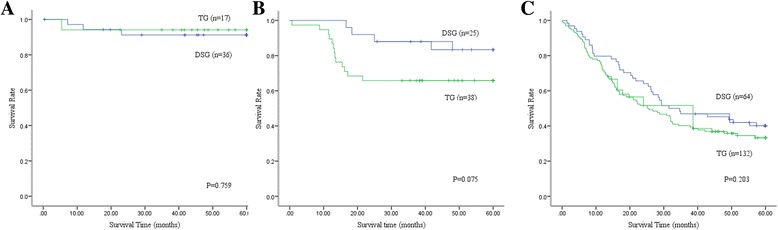
Results: We collect data of 339 patients between January 2005 and October 2011. A total of 144 patients underwent distal subtotal gastrectomy, and 195 patients underwent total gastrectomy. Patients in the total gastrectomy group have longer operative duration (P < 0.001) and postoperative hospital stay (P = 0.001) than those in the distal subtotal gastrectomy group. In the total gastrectomy group, more lymph nodes are harvested (P < 0.001). Meanwhile, the rate of postoperative complications is lower in the distal subtotal gastrectomy group than in the total gastrectomy group (8% vs 15%, P = 0.047). Further analysis demonstrates that the rate of anastomosis leakage is lower in the distal subtotal gastrectomy group than in the total gastrectomy group (0% vs 4%, P = 0.023). Kaplan-Meier (log rank test) analysis shows a significant difference in overall survival between the two groups. The 5-year overall survival rates in the distal subtotal gastrectomy and total gastrectomy groups are 65% and 47%, respectively (P < 0.001). Further stage-stratified analysis reveals that no statistical significance exists in 5-year survival rate between the distal subtotal gastrectomy and total gastrectomy groups at the same stage. Multivariate analysis shows that age (P = 0.046), operation duration (P < 0.001), complications (P = 0.037), usage of neoadjuvant chemotherapy (P < 0.001), tumor size (P = 0.012), presence of lymphovascular invasion (P = 0.043) and N stage (P < 0.001) are independent prognostic factors for survival.
Conclusions: For patients with middle-third gastric cancer, distal subtotal gastrectomy shortens the operation duration and postoperative hospital stay and reduces postoperative complications. Meanwhile, the long-term survival of patients with distal subtotal gastrectomy is similar to that of those with total gastrectomy at the same stage. The extent of gastrectomy for middle-third gastric cancer is not an independent prognostic factor for survival.
Keywords: Distal subtotal gastrectomy; Middle-third gastric cancer; Overall survival; Total gastrectomy.
Figures
References
-
- Van Cutsem E, Dicato M, Geva R, Arber N, Bang Y, Benson A, et al. The diagnosis and management of gastric cancer: expert discussion and recommendations from the 12th ESMO/World Congress on Gastrointestinal Cancer, Barcelona, 2010. Ann Oncol. 2011;22(Suppl 5):v1–v9. doi: 10.1093/annonc/mdr284. - DOI - PubMed
-
- Lutz MP, Zalcberg JR, Ducreux M, Ajani JA, Allum W, Aust D, et al. Highlights of the EORTC St. Gallen International Expert Consensus on the primary therapy of gastric, gastroesophageal and oesophageal cancer - differential treatment strategies for subtypes of early gastroesophageal cancer. Eur J Cancer. 2012;48(16):2941–2953. doi: 10.1016/j.ejca.2012.07.029. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
