

Comparison of fluid balance and hemodynamic and metabolic effects of sodium lactate versus sodium bicarbonate versus 0.9% NaCl in porcine endotoxic shock: a randomized, open-label, controlled study
- PMID: 28526086
- PMCID: PMC5438514
- DOI: 10.1186/s13054-017-1694-1
Comparison of fluid balance and hemodynamic and metabolic effects of sodium lactate versus sodium bicarbonate versus 0.9% NaCl in porcine endotoxic shock: a randomized, open-label, controlled study
Abstract
Background: Sodium lactate has been shown to improve hemodynamics and avoid fluid overload. The objective of this study was to confirm a beneficial effect on fluid balance with sodium lactate infusion and to specify whether the advantage of lactate is related to a negative chloride balance, its particular metabolism, or simply its energy load.
Methods: This was an interventional, randomized, open-label, controlled experimental study. Fifteen female "large white" pigs (2 months old) were challenged with intravenous infusion of Escherichia coli endotoxin. Three groups of five animals were randomly assigned to receive different fluids: a treatment group received sodium lactate 11.2% (SL group); an isotonic control group received 0.9% NaCl (NC group); and a hypertonic control group, with the same amount of osmoles and sodium as the SL group, received sodium bicarbonate 8.4% (SB group). In order to provide the same energy load in the three groups, control groups were perfused with an equivalent energy supply. Statistical analysis was performed with non-parametric tests and the Dunn correction for multiple comparisons at p < 0.05.
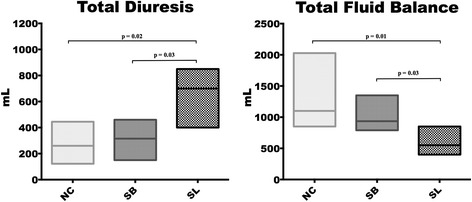
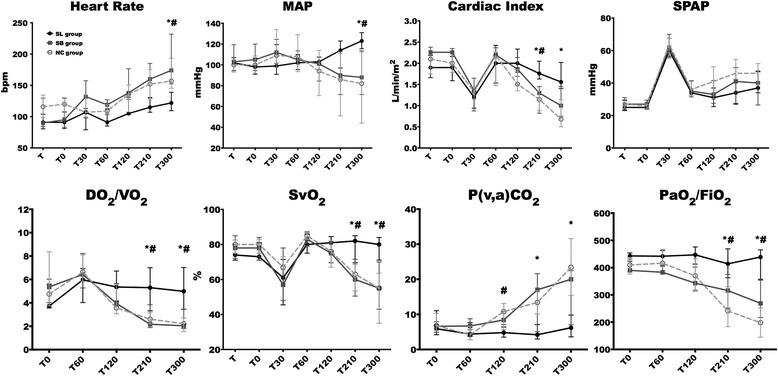
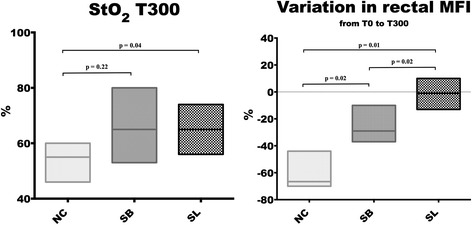
Results: Fluid and chloride balance, hemodynamics, oxygenation markers, and microcirculatory parameters were measured over a 5-h period. Cumulative fluid balance was significantly lower in the SL group (550 (415-800) mL; median (interquartile range)) compared to the NC group (1100 (920-1640) mL, p = 0.01) and the SB group (935 (790-1220) mL, p = 0.03). Hemodynamics, cardiac efficiency, and microcirculation were significantly enhanced in the SL group, resulting in a significant improvement in oxygen delivery (SL group 417 (305-565) mL/min/m2 at 300 min versus the NC (207 (119-272) mL/min/m2, p = 0.01) and the SB (278, (211-315) mL/min/m2, p = 0.03) groups). Oxygenation markers (arterial oxygen partial pressure (PaO2)/inspired oxygen fraction (FiO2), mixed venous oxygen saturation (SvO2), and venoarterial carbon dioxide tension difference (Pv-aCO2) were enhanced with sodium lactate infusion. Chloride balance was equivalent in both hypertonic groups and significantly reduced compared to the NC group.
Conclusion: Sodium lactate infusion improves fluid balance and hemodynamics. The advantage of lactate does not seem to be explained by its energy load or by the induced negative chloride balance with subsequent water movements.
Keywords: Fluid balance; Lactate infusion; Metabolism; Microcirculation; Organ failure; Septic shock.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
