

Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial
- PMID: 28526536
- PMCID: PMC5531181
- DOI: 10.1016/S1470-2045(17)30312-1
Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial
Erratum in
-
Correction to Lancet Oncol 2017; 18: 732-42.Lancet Oncol. 2017 Aug;18(8):e433. doi: 10.1016/S1470-2045(17)30527-2. Epub 2017 Jul 26. Lancet Oncol. 2017. PMID: 28759383 No abstract available.
-
Correction to Lancet Oncol 2017; 18: 732-42.Lancet Oncol. 2018 Dec;19(12):e667. doi: 10.1016/S1470-2045(18)30848-9. Lancet Oncol. 2018. PMID: 30507428 No abstract available.
Abstract
Background: The antibody-drug conjugate trastuzumab emtansine is indicated for the treatment of patients with HER2-positive metastatic breast cancer previously treated with trastuzumab and a taxane. Approval of this drug was based on progression-free survival and interim overall survival data from the phase 3 EMILIA study. In this report, we present a descriptive analysis of the final overall survival data from that trial.
Methods: EMILIA was a randomised, international, open-label, phase 3 study of men and women aged 18 years or older with HER2-positive unresectable, locally advanced or metastatic breast cancer previously treated with trastuzumab and a taxane. Enrolled patients were randomly assigned (1:1) via a hierarchical, dynamic randomisation scheme and an interactive voice response system to trastuzumab emtansine (3·6 mg/kg intravenously every 3 weeks) or control (capecitabine 1000 mg/m2 self-administered orally twice daily on days 1-14 on each 21-day cycle, plus lapatinib 1250 mg orally once daily on days 1-21). Randomisation was stratified by world region (USA vs western Europe vs or other), number of previous chemotherapy regimens for unresectable, locally advanced, or metastatic disease (0 or 1 vs >1), and disease involvement (visceral vs non-visceral). The coprimary efficacy endpoints were progression-free survival (per independent review committee assessment) and overall survival. Efficacy was analysed in the intention-to-treat population; safety was analysed in all patients who received at least one dose of study treatment, with patients analysed according to the treatment actually received. On May 30, 2012, the study protocol was amended to allow crossover from control to trastuzumab emtansine after the second interim overall survival analysis crossed the prespecified overall survival efficacy boundary. This study is registered with ClinicalTrials.gov, number NCT00829166.
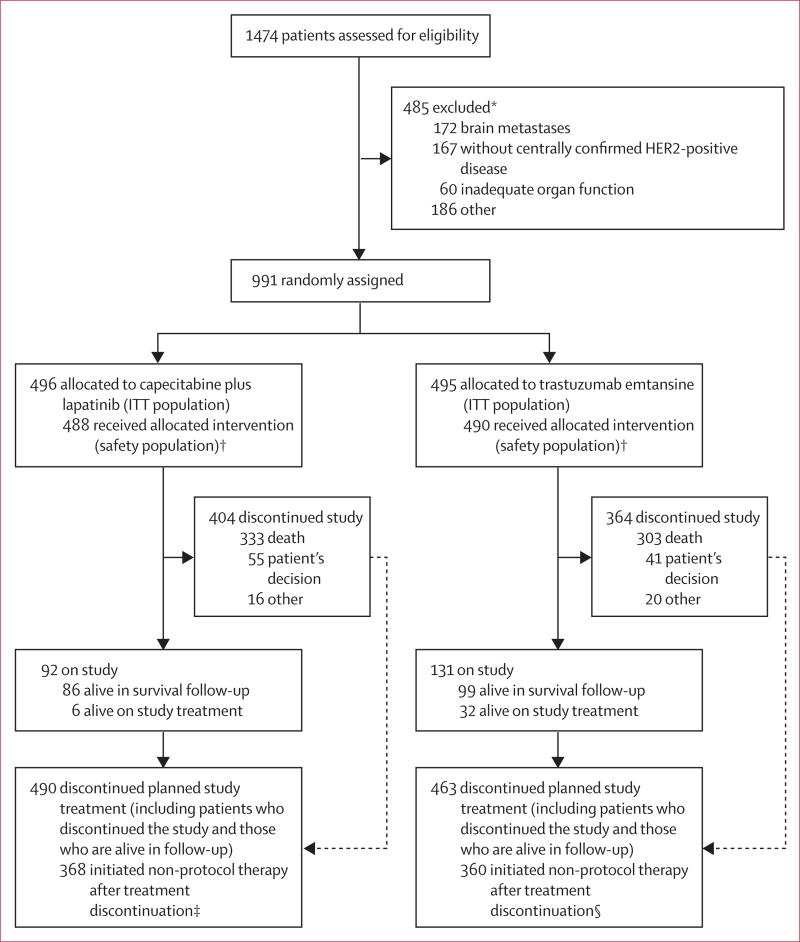
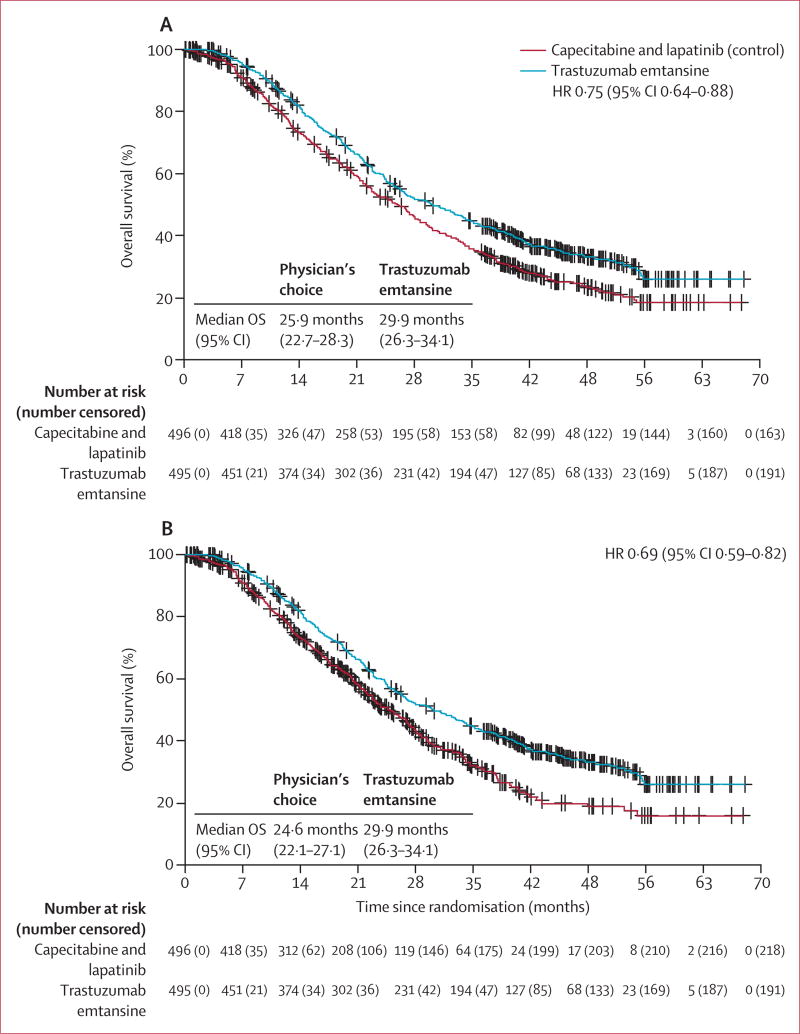
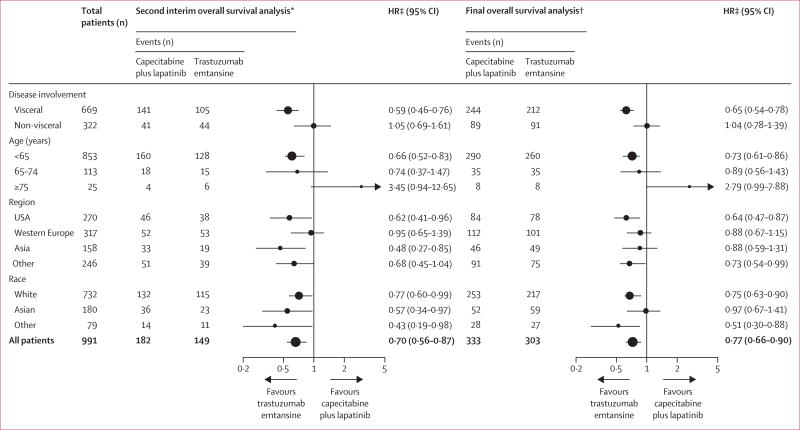
Findings: Between Feb 23, 2009, and Oct 13, 2011, 991 eligible patients were enrolled and randomly assigned to either trastuzumab emtansine (n=495) or capecitabine and lapatinib (control; n=496). In this final descriptive analysis, median overall survival was longer with trastuzumab emtansine than with control (29·9 months [95% CI 26·3-34·1] vs 25·9 months [95% CI 22·7-28·3]; hazard ratio 0·75 [95% CI 0·64-0·88]). 136 (27%) of 496 patients crossed over from control to trastuzumab emtansine after the second interim overall survival analysis (median follow-up duration 24·1 months [IQR 19·5-26·1]). Of those patients originally randomly assigned to trastuzumab emtansine, 254 (51%) of 495 received capecitabine and 241 [49%] of 495 received lapatinib (separately or in combination) after study drug discontinuation. In the safety population (488 patients treated with capecitabine plus lapatinib, 490 patients treated with trastuzumab emtansine), fewer grade 3 or worse adverse events occurred with trastuzumab emtansine (233 [48%] of 490) than with capecitabine plus lapatinib control treatment (291 [60%] of 488). In the control group, the most frequently reported grade 3 or worse adverse events were diarrhoea (103 [21%] of 488 patients) followed by palmar-plantar erythrodysaesthesia syndrome (87 [18%]), and vomiting (24 [5%]). The safety profile of trastuzumab emtansine was similar to that reported previously; the most frequently reported grade 3 or worse adverse events in the trastuzumab emtansine group were thrombocytopenia (70 [14%] of 490), increased aspartate aminotransferase levels (22 [5%]), and anaemia (19 [4%]). Nine patients died from adverse events; five of these deaths were judged to be related to treatment (two in the control group [coronary artery disease and multiorgan failure] and three in the trastuzumab emtansine group [metabolic encephalopathy, neutropenic sepsis, and acute myeloid leukaemia]).
Interpretation: This descriptive analysis of final overall survival in the EMILIA trial shows that trastuzumab emtansine improved overall survival in patients with previously treated HER2-positive metastatic breast cancer even in the presence of crossover treatment. The safety profile was similar to that reported in previous analyses, reaffirming trastuzumab emtansine as an efficacious and tolerable treatment in this patient population.
Funding: F Hoffmann-La Roche/Genentech.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Conflict of interest statement
VD has served as a consultant for F Hoffmann-La Roche/Genentech, Novartis/GlaxoSmithKline, Abbvie, and Pfizer. DM has served as a consultant for F Hoffmann-La Roche/Genentech. MP has served as a consultant for Genentech. His institution has received research support from Genentech. MW has served as a consultant for F Hoffmann-La Roche, Novartis, AstraZeneca, Janssen, Lilly, and Bristol-Myers Squibb. IEK’s institution has received research support from Genentech. KB has served as a consultant for F Hoffmann-La Roche/Genentech, Novartis, Puma, Amgen, AstraZeneca, Celgene, Eli Lilly, Eisai, GE Healthcare, Hospira, Pfizer, Rockwell, Spectrum, Incyte, Sandoz, Janssen, and Bayer. KB has also received research support from Genentech, Novartis, Pfizer, and Celgene. SH is an employee of CRO KOEHLER-eClinical, which was contracted to work on behalf of F Hoffmann-La Roche. JX and MG are salaried employees of Genentech and own stock in F Hoffmann-La Roche. LG has received consulting fees from F Hoffmann-La Roche/Genentech, GlaxoSmithKline, Novartis, Pfizer, Boehringer Ingelheim, Celgene, Tahio, Onkaido, and Tiziana. SV and JB declare no competing interests.
Figures
Comment in
-
Trastuzumab emtansine in HER2-positive metastatic breast cancer.Lancet Oncol. 2017 Jun;18(6):696-697. doi: 10.1016/S1470-2045(17)30303-0. Epub 2017 May 16. Lancet Oncol. 2017. PMID: 28526537 No abstract available.
-
Breast cancer: T-DM1 - an important agent in the history of breast cancer management.Nat Rev Clin Oncol. 2017 Nov;14(11):651-652. doi: 10.1038/nrclinonc.2017.123. Epub 2017 Aug 8. Nat Rev Clin Oncol. 2017. PMID: 28786416 No abstract available.
References
-
- Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235:177–82. - PubMed
-
- Ross JS, Slodkowska EA, Symmans WF, Pusztai L, Ravdin PM, Hortobagyi GN. The HER-2 receptor and breast cancer: ten years of targeted anti-HER-2 therapy and personalized medicine. Oncologist. 2009;14:320–68. - PubMed
-
- Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344:783–92. - PubMed
-
- Marty M, Cognetti F, Maraninchi D, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 Study Group. J Clin Oncol. 2005;23:4265–74. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
