

Evaluation of crescent formation as a predictive marker in immunoglobulin A nephropathy: a systematic review and meta-analysis
- PMID: 28526805
- PMCID: PMC5542279
- DOI: 10.18632/oncotarget.17502
Evaluation of crescent formation as a predictive marker in immunoglobulin A nephropathy: a systematic review and meta-analysis
Abstract
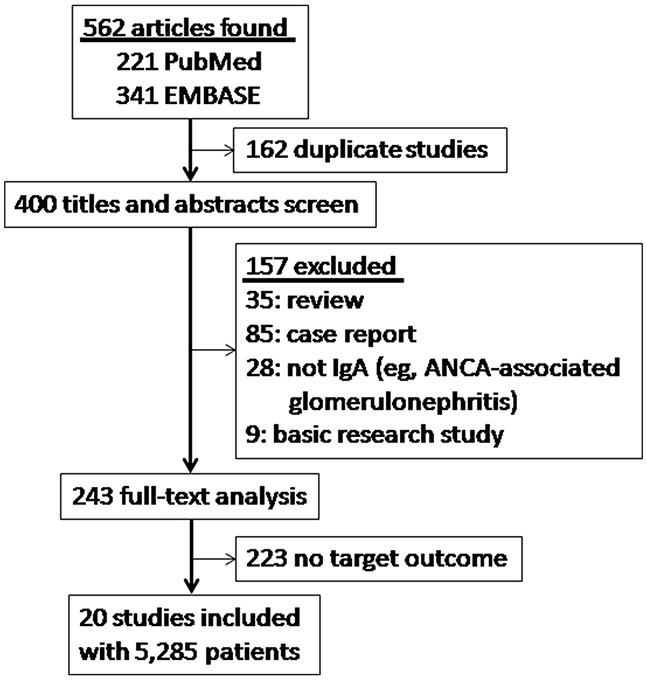
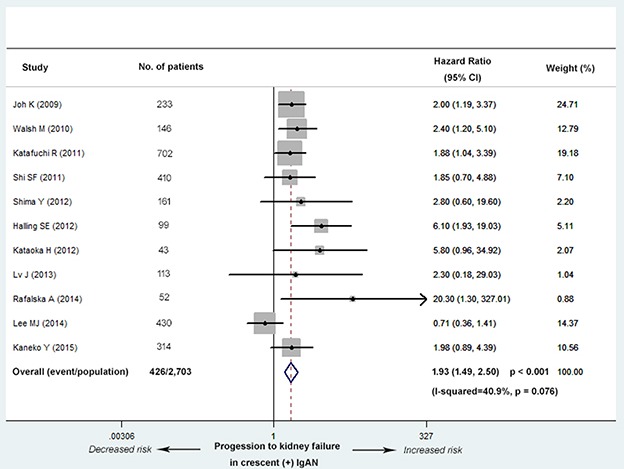
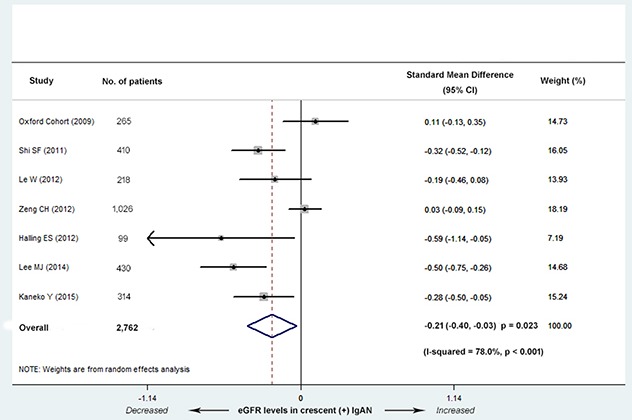
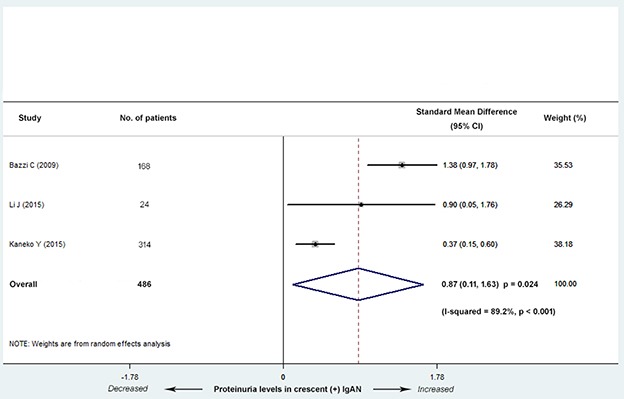
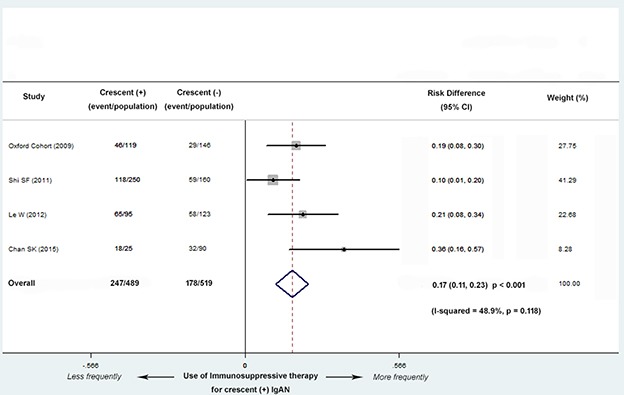
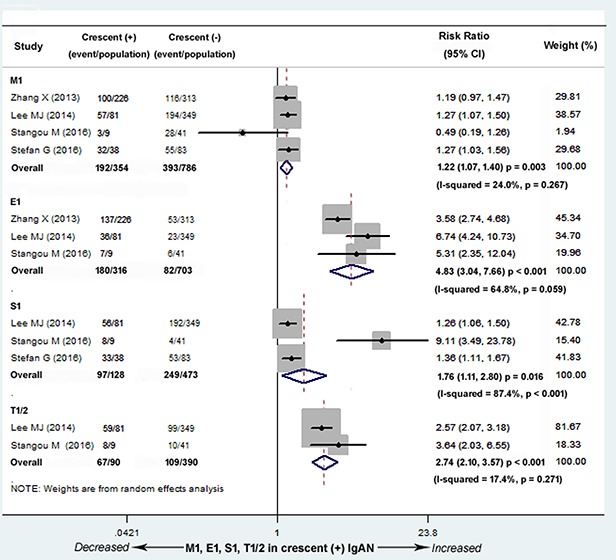
The 2009 Oxford Classification of immunoglobulin A (IgA) nephropathy (IgAN) identifies four histological features as predictors of renal prognosis: mesangial hypercellularity (M), endocapillary hypercellularity (E), segmental glomerulosclerosis (S), and tubular atrophy/interstitial fibrosis (T). However, the clinical and prognostic significance of crescent formation still remains controversial. Therefore, we performed a meta-analysis to evaluate the association between crescents and kidney outcome in IgAN. A total of 20 studies published from January 2009 to July 2016 involving 5,285 patients were included after systematic searches of PubMed and EMBASE databases. Pooled results showed that crescent lesions were associated with kidney failure (HR, 1.93; 95% CI, 1.49-2.50; P < 0.001). IgAN patients with crescents had lower eGFR levels (SMD, -0.21; 95% CI, -0.40--0.03; P = 0.023); higher proteinuria levels (SMD, 0.87; 95% CI, 0.11-1.63; P = 0.024); a larger number of patients with M1 (RR, 1.22; 95% CI, 1.07-1.40; P = 0.003), E1 (RR, 4.83; 95% CI, 3.04-7.66;P < 0.001), S1 (RR, 1.76; 95% CI, 1.11-2.80; P = 0.016) and T1/2 (RR, 2.74; 95% CI, 2.10-3.57; P < 0.001) lesions; and received immunosuppressive therapy more frequently (RD, 0.17; 95% CI, 0.11-0.23; P < 0.001). Our results suggest that crescent formation represents an efficient prognostic factor associated with progression to kidney failure and thus could be considered into the new Oxford Classification.
Keywords: Immunoglobulin A (IgA) nephropathy; crescent lesions; meta-analysis; oxford classification.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Evaluation of the Oxford Classification of IgA nephropathy: a systematic review and meta-analysis.Am J Kidney Dis. 2013 Nov;62(5):891-9. doi: 10.1053/j.ajkd.2013.04.021. Epub 2013 Jun 29. Am J Kidney Dis. 2013. PMID: 23820066
-
Global glomerulosclerosis proportions predict nephropathy progression in IgA nephropathy: a multicenter retrospective analysis with propensity score matching.Ren Fail. 2025 Dec;47(1):2486567. doi: 10.1080/0886022X.2025.2486567. Epub 2025 May 5. Ren Fail. 2025. PMID: 40325551 Free PMC article.
-
Combined Effects of the Serum IgA/C3 Ratio and Glomerular C3 Staining on the Renal Outcome in Adult Immunoglobulin A Nephropathy.Kidney Blood Press Res. 2024;49(1):246-257. doi: 10.1159/000536114. Epub 2024 Feb 21. Kidney Blood Press Res. 2024. PMID: 38382485
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Serum IgA/C3 ratio as a diagnostic and prognostic biomarker for IgA nephropathy.Sci Rep. 2025 Aug 8;15(1):29007. doi: 10.1038/s41598-025-10578-x. Sci Rep. 2025. PMID: 40781100 Free PMC article.
Cited by
-
Analysis of Various Types of Glomerulonephritis with Crescents at a Single Center.Int J Nephrol. 2022 May 9;2022:1749548. doi: 10.1155/2022/1749548. eCollection 2022. Int J Nephrol. 2022. PMID: 35586040 Free PMC article.
-
Formalin-fixed paraffin-embedded renal biopsy tissues: an underexploited biospecimen resource for gene expression profiling in IgA nephropathy.Sci Rep. 2020 Sep 16;10(1):15164. doi: 10.1038/s41598-020-72026-2. Sci Rep. 2020. PMID: 32938960 Free PMC article.
-
Crescents and IgA Nephropathy: A Delicate Marriage.J Clin Med. 2022 Jun 21;11(13):3569. doi: 10.3390/jcm11133569. J Clin Med. 2022. PMID: 35806856 Free PMC article. Review.
-
A Novel Scoring System Based on Oxford Classification Indicating Steroid Therapy Use for IgA Nephropathy.Kidney Int Rep. 2021 Oct 14;7(1):99-107. doi: 10.1016/j.ekir.2021.10.007. eCollection 2022 Jan. Kidney Int Rep. 2021. PMID: 35005318 Free PMC article.
-
Nomogram for the prediction of crescent formation in IgA nephropathy patients: a retrospective study.BMC Nephrol. 2023 Sep 4;24(1):262. doi: 10.1186/s12882-023-03310-2. BMC Nephrol. 2023. PMID: 37667217 Free PMC article.
References
-
- Koyama A, Igarashi M, Kobayashi M. Natural history and risk factors for immunoglobulin A nephropathy in Japan. Research Group on Progressive Renal Diseases. Am J Kidney Dis. 1997;29:526–32. - PubMed
-
- Roberts IS, Cook HT, Troyanov S, Alpers CE, Amore A, Barratt J, Berthoux F, Bonsib S, Bruijn JA, Cattran DC, Coppo R, D'Agati V, D'Amico G, et al. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. 2009;76:546–56. doi: 10.1038/ki.2009.168. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
