

Long-term follow-up after near-infrared fluorescence-guided resection of colorectal liver metastases: A retrospective multicenter analysis
- PMID: 28528189
- PMCID: PMC5534212
- DOI: 10.1016/j.ejso.2017.04.016
Long-term follow-up after near-infrared fluorescence-guided resection of colorectal liver metastases: A retrospective multicenter analysis
Abstract
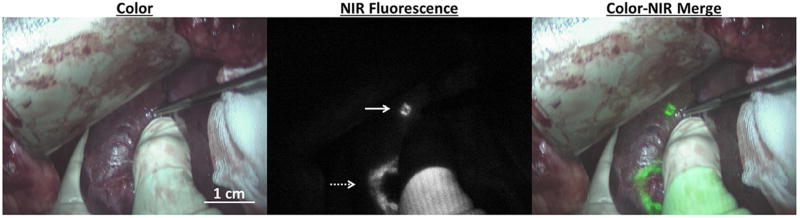
Background: Several studies demonstrated that intraoperative near-infrared fluorescence (NIRF) imaging using indocyanine green (ICG) identifies (sub)capsular colorectal liver metastases (CRLM) missed by other techniques. It is unclear if this results in any survival benefit. This study evaluates long-term follow-up after NIRF-guided resection of CRLM using ICG.
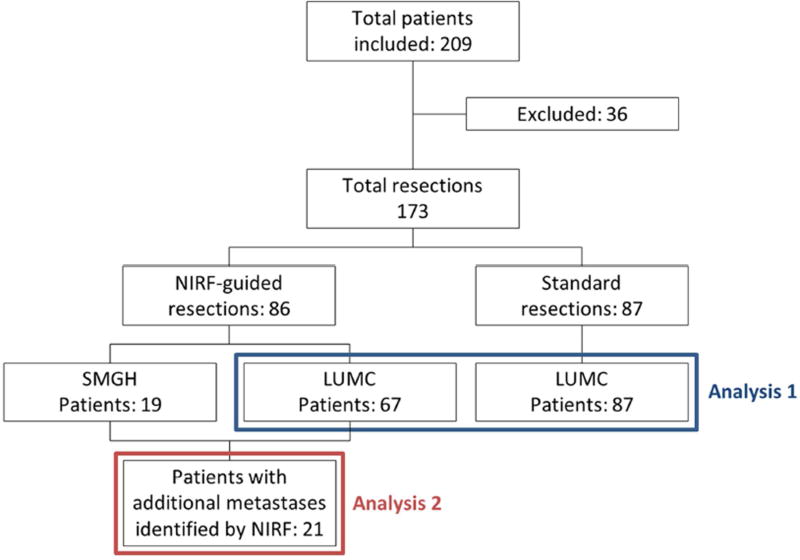
Methods: First, patients undergoing resection of CRLM with or without NIRF imaging were analyzed retrospectively. Perioperative details, liver-specific recurrence-free interval and overall survival were compared. Second, the prognosis of patients in whom additional metastases were identified solely by NIRF was studied.
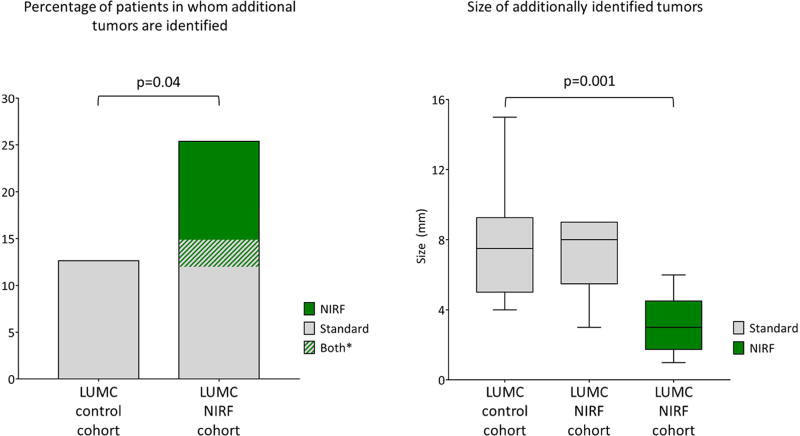
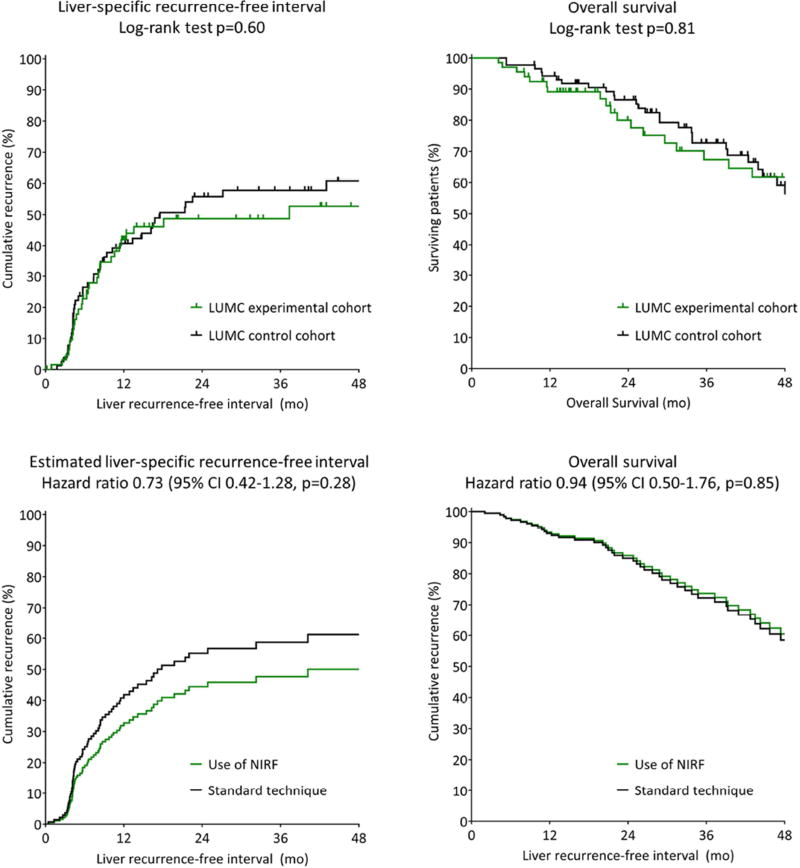
Results: Eighty-six patients underwent resection with NIRF imaging and 87 without. In significantly more patients of the NIRF imaging cohort additional metastases were identified during surgery (25% vs. 13%, p = 0.04). Tumors identified solely by NIRF imaging were significantly smaller compared to additional metastases identified also by inspection, palpation or intraoperative ultrasound (3.2 ± 1.8 mm vs. 7.4 ± 2.6 mm, p < 0.001). Liver-specific recurrence-free survival at 4 years was 47% with NIRF imaging and 39% without (hazard ratio at multivariate analysis 0.73, 95% CI 0.42-1.28, p = 0.28). Overall survival at 4 years was 62% and 59%, respectively (p = 0.79). No liver recurrences occurred within 3 years follow-up in 52% of patients in whom additional metastases were resected based on only NIRF imaging.
Conclusions: This study suggests that NIRF imaging identifies significantly more and smaller tumors during resection of CRLM, preventing recurrences in a subset of patients. Given its safety profile and low expense, routine use can be considered until tumor targeting fluorescent tracers are clinically available.
Keywords: Cancer; Fluorescence imaging; Indocyanine green; Liver neoplasms; Prognosis; Surgery.
Copyright © 2017 Elsevier Ltd, BASO ~ The Association for Cancer Surgery, and the European Society of Surgical Oncology. All rights reserved.
Conflict of interest statement
Figures
References
-
- Wei AC, et al. Survival after hepatic resection for colorectal metastases: a 10-year experience. Ann Surg Oncol. 2006;13:668–76. - PubMed
-
- Rees M, et al. Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer: a multifactorial model of 929 patients. Ann Surg. 2008;247:125–35. - PubMed
-
- Karanjia ND, et al. Survival and recurrence after neo-adjuvant chemotherapy and liver resection for colorectal metastases: a ten year study. Eur J Surg Oncol. 2009;35:838–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
