

Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
- PMID: 28528569
- PMCID: PMC5538258
- DOI: 10.1056/NEJMoa1703058
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
Abstract
Background: In 2013, New York began requiring hospitals to follow protocols for the early identification and treatment of sepsis. However, there is controversy about whether more rapid treatment of sepsis improves outcomes in patients.
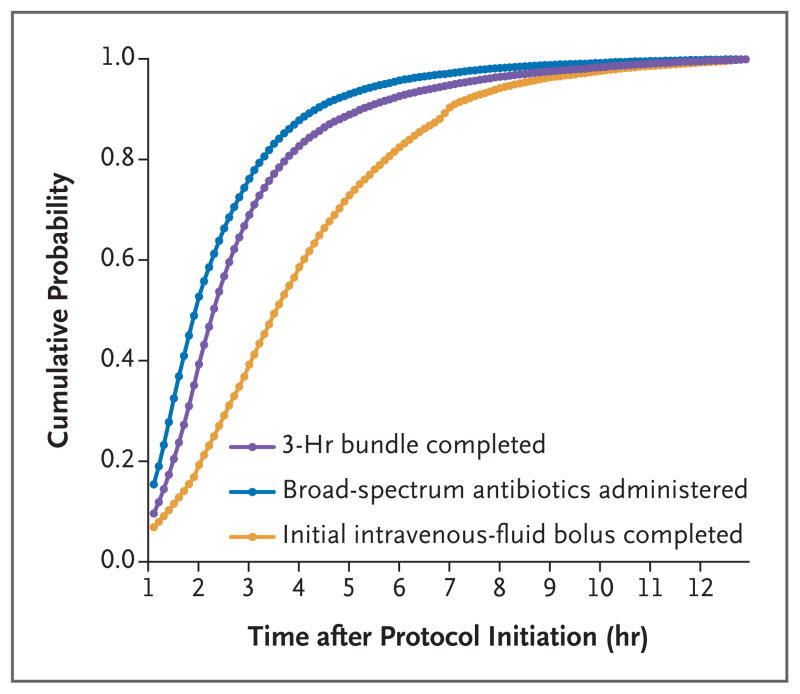
Methods: We studied data from patients with sepsis and septic shock that were reported to the New York State Department of Health from April 1, 2014, to June 30, 2016. Patients had a sepsis protocol initiated within 6 hours after arrival in the emergency department and had all items in a 3-hour bundle of care for patients with sepsis (i.e., blood cultures, broad-spectrum antibiotic agents, and lactate measurement) completed within 12 hours. Multilevel models were used to assess the associations between the time until completion of the 3-hour bundle and risk-adjusted mortality. We also examined the times to the administration of antibiotics and to the completion of an initial bolus of intravenous fluid.
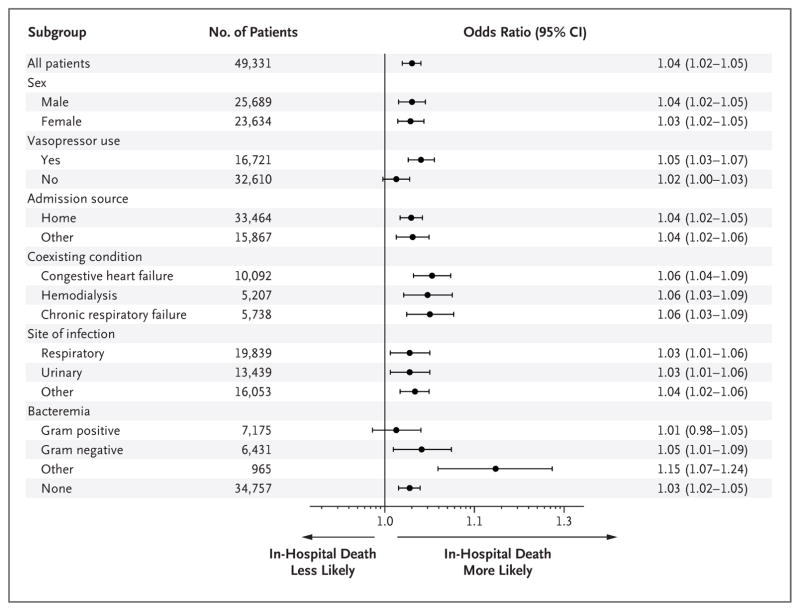
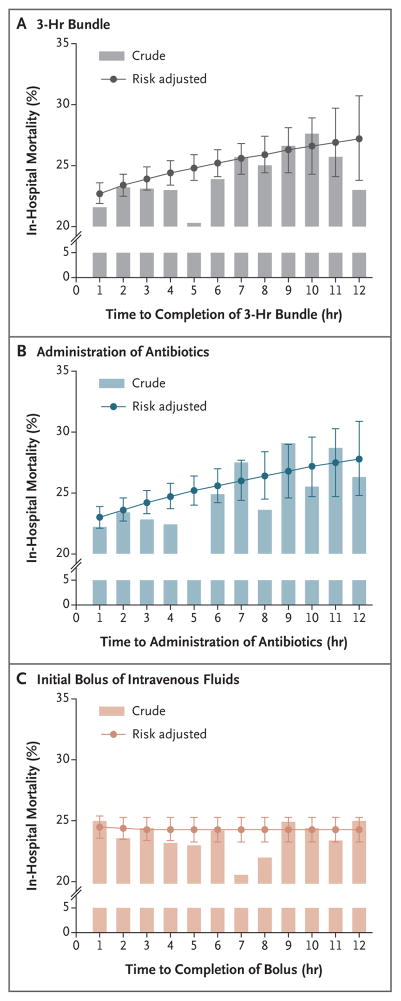
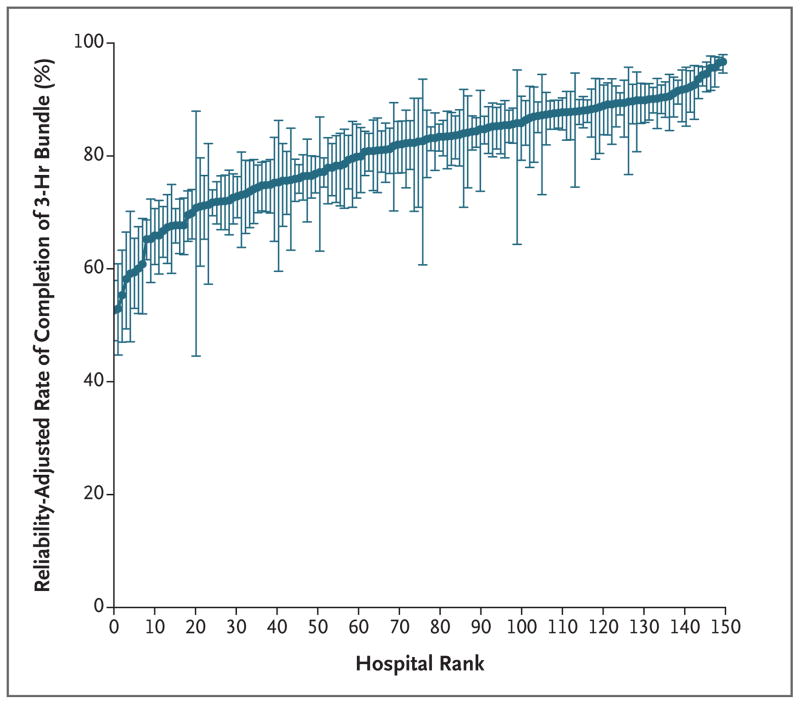
Results: Among 49,331 patients at 149 hospitals, 40,696 (82.5%) had the 3-hour bundle completed within 3 hours. The median time to completion of the 3-hour bundle was 1.30 hours (interquartile range, 0.65 to 2.35), the median time to the administration of antibiotics was 0.95 hours (interquartile range, 0.35 to 1.95), and the median time to completion of the fluid bolus was 2.56 hours (interquartile range, 1.33 to 4.20). Among patients who had the 3-hour bundle completed within 12 hours, a longer time to the completion of the bundle was associated with higher risk-adjusted in-hospital mortality (odds ratio, 1.04 per hour; 95% confidence interval [CI], 1.02 to 1.05; P<0.001), as was a longer time to the administration of antibiotics (odds ratio, 1.04 per hour; 95% CI, 1.03 to 1.06; P<0.001) but not a longer time to the completion of a bolus of intravenous fluids (odds ratio, 1.01 per hour; 95% CI, 0.99 to 1.02; P=0.21).
Conclusions: More rapid completion of a 3-hour bundle of sepsis care and rapid administration of antibiotics, but not rapid completion of an initial bolus of intravenous fluids, were associated with lower risk-adjusted in-hospital mortality. (Funded by the National Institutes of Health and others.).
Figures
Comment in
-
In sepsis, beyond adherence, timeliness matters.J Thorac Dis. 2017 Sep;9(9):2808-2811. doi: 10.21037/jtd.2017.08.65. J Thorac Dis. 2017. PMID: 29221245 Free PMC article. No abstract available.
-
From Barcelona to New York: 15 years of transition of sepsis performance improvement.J Thorac Dis. 2017 Oct;9(10):3453-3455. doi: 10.21037/jtd.2017.08.144. J Thorac Dis. 2017. PMID: 29268313 Free PMC article. No abstract available.
-
Sepsis Therapies: Insights from Population Health to Cellular Therapies and Genomic Medicine.Am J Respir Crit Care Med. 2018 Dec 15;198(12):1570-1572. doi: 10.1164/rccm.201804-0782RR. Am J Respir Crit Care Med. 2018. PMID: 30277812 Free PMC article. No abstract available.
References
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41:1167–74. - PubMed
-
- Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43:304–77. - PubMed
-
- Kumar A, Haery C, Paladugu B, et al. The duration of hypotension before the initiation of antibiotic treatment is a critical determinant of survival in a murine model of Escherichia coli septic shock: association with serum lactate and inflammatory cytokine levels. J Infect Dis. 2006;193:251–8. - PubMed
-
- Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42:1749–55. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous