

Treatment of the Mal de Debarquement Syndrome: A 1-Year Follow-up
- PMID: 28529496
- PMCID: PMC5418223
- DOI: 10.3389/fneur.2017.00175
Treatment of the Mal de Debarquement Syndrome: A 1-Year Follow-up
Abstract
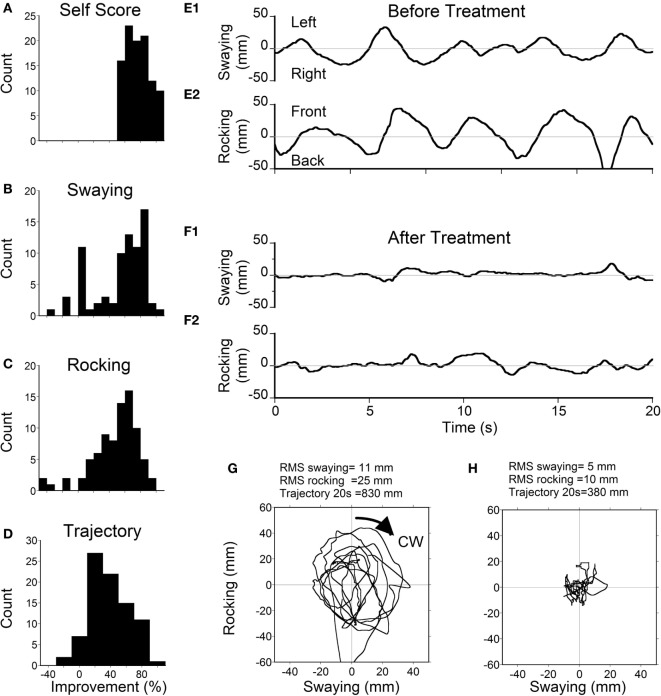
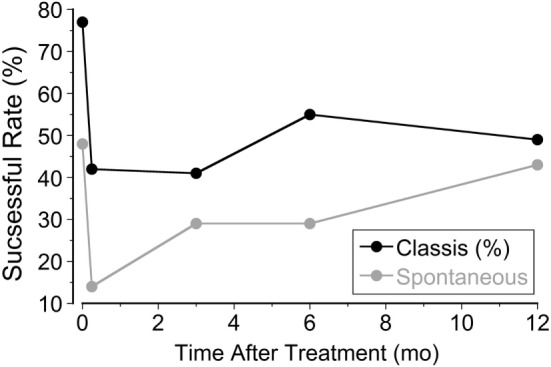
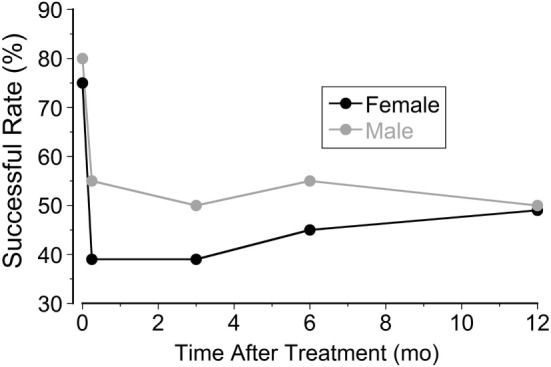
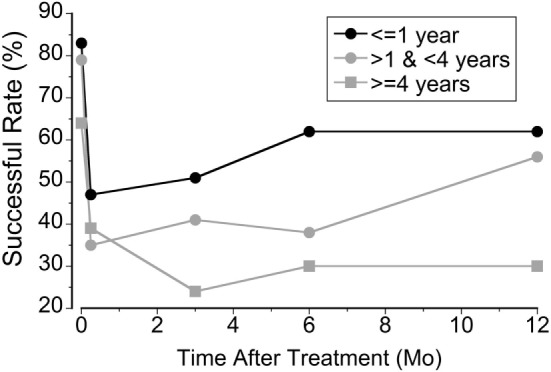
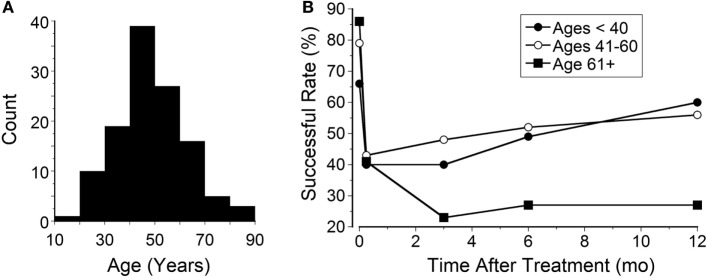
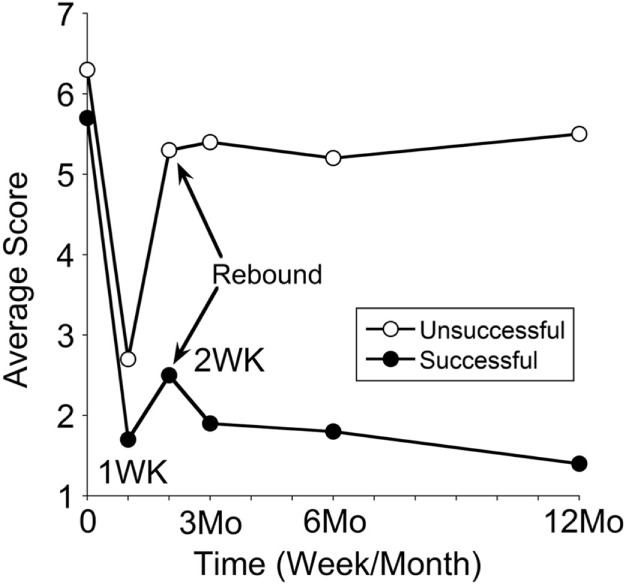
The mal de debarquement syndrome (MdDS) is a movement disorder, occurring predominantly in women, is most often induced by passive transport on water or in the air (classic MdDS), or can occur spontaneously. MdDS likely originates in the vestibular system and is unfamiliar to many physicians. The first successful treatment was devised by Dai et al. (1), and over 330 MdDS patients have now been treated. Here, we report the outcomes of 141 patients (122 females and 19 males) treated 1 year or more ago. We examine the patient's rocking frequency, body drifting, and nystagmus. The patients are then treated according to these findings for 4-5 days. During treatment, patients' heads were rolled while watching a rotating full-field visual surround (1). Their symptom severity after the initial treatment and at the follow-up was assessed using a subjective 10-point scale. Objective measures, taken before and at the end of the week of treatment, included static posturography. Significant improvement was a reduction in symptom severity by more than 50%. Objective measures were not possible during the follow-up because of the wide geographic distribution of the patients. The treatment group consisted of 120 classic and 21 spontaneous MdDS patients. The initial rate of significant improvement after a week of treatment was 78% in classic and 48% in spontaneous patients. One year later, significant improvement was maintained in 52% of classic and 48% of spontaneous subjects. There was complete remission of symptoms in 27% (32) of classic and 19% (4) of spontaneous patients. Although about half of them did not achieve a 50% improvement, most reported fewer and milder symptoms than before. The success of the treatment was generally inversely correlated with the duration of the MdDS symptoms and with the patients' ages. Prolonged travel by air or car on the way home most likely contributed to the symptomatic reversion from the initial successful treatment. Our results indicate that early diagnosis and treatment can significantly improve results, and the prevention of symptomatic reversion will increase the long-term benefit in this disabling disorder.
Keywords: adaptation; bobbing; disembarking syndrome; rocking; sea legs; swaying; velocity storage; vestibular.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials