

Ceramic Biocomposites as Biodegradable Antibiotic Carriers in the Treatment of Bone Infections
- PMID: 28529863
- PMCID: PMC5423569
- DOI: 10.7150/jbji.17234
Ceramic Biocomposites as Biodegradable Antibiotic Carriers in the Treatment of Bone Infections
Abstract
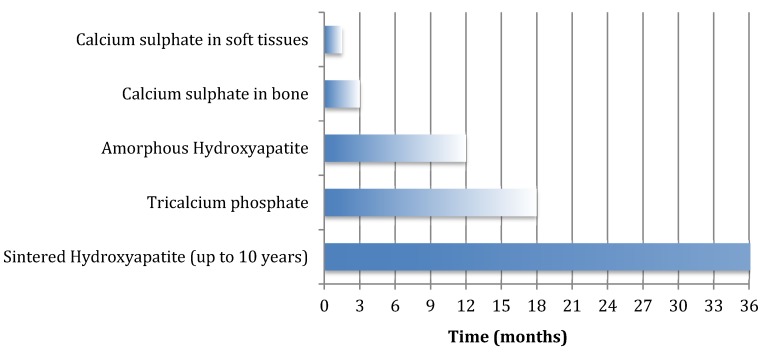
Local release of antibiotic has advantages in the treatment of chronic osteomyelitis and infected fractures. The adequacy of surgical debridement is still key to successful clearance of infection but local antibiotic carriers seem to afford greater success rates by targeting the residual organisms present after debridement and delivering much higher local antibiotic concentrations compared with systemic antibiotics alone. Biodegradable ceramic carriers can be used to fill osseous defects, which reduces the dead space and provides the potential for subsequent repair of the osseous defect as they dissolve away. A dissolving ceramic antibiotic carrier also raises the possibility of single stage surgery with definitive closure and avoids the need for subsequent surgery for spacer removal. In this article we provide an overview of the properties of various biodegradable ceramics, including calcium sulphate, the calcium orthophosphate ceramics, calcium phosphate cement and polyphasic carriers. We summarise the antibiotic elution properties as investigated in previous animal studies as well as the clinical outcomes from clinical research investigating their use in the surgical management of chronic osteomyelitis. Calcium sulphate pellets have been shown to be effective in treating local infection, although newer polyphasic carriers may support greater osseous repair and reduce the risk of further fracture or the need for secondary reconstructive surgery. The use of ceramic biocomposites to deliver antibiotics together with BMPs, bisphosphonates, growth factors or living cells is under investigation and merits further study. We propose a treatment protocol, based on the Cierny-Mader classification, to help guide the appropriate selection of a suitable ceramic antibiotic carrier in the surgical treatment of chronic osteomyelitis.
Keywords: Osteomyelitis; antibiotic carrier; biodegradable; calcium phosphate.; calcium sulphate; ceramic.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Trampuz A, Zimmerli DW. Antimicrobial agents in orthopaedic surgery. Drugs. 2006;66(8):1089–106. - PubMed
-
- Brady RA, Leid JG, Calhoun JH, Costerton JW, Shirtliff ME. Osteomyelitis and the role of biofilms in chronic infection. Federation of European Microbiological Societies Immunology & Medical Microbiology. 2008;52(1):13–22. - PubMed
-
- Cierny G, Mader JT, Penninck JJ. The classic: A clinical staging system for adult osteomyelitis. Clinical Orthopaedics & Related Research. 2003;414:7–24. - PubMed
-
- McNally M, Nagarajah K. Osteomyelitis. Orthopaedics and Trauma. 2010;24(6):416–29.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
