

Where do HIV-infected adolescents go after transfer? - Tracking transition/transfer of HIV-infected adolescents using linkage of cohort data to a health information system platform
- PMID: 28530037
- PMCID: PMC5577779
- DOI: 10.7448/IAS.20.4.21668
Where do HIV-infected adolescents go after transfer? - Tracking transition/transfer of HIV-infected adolescents using linkage of cohort data to a health information system platform
Abstract
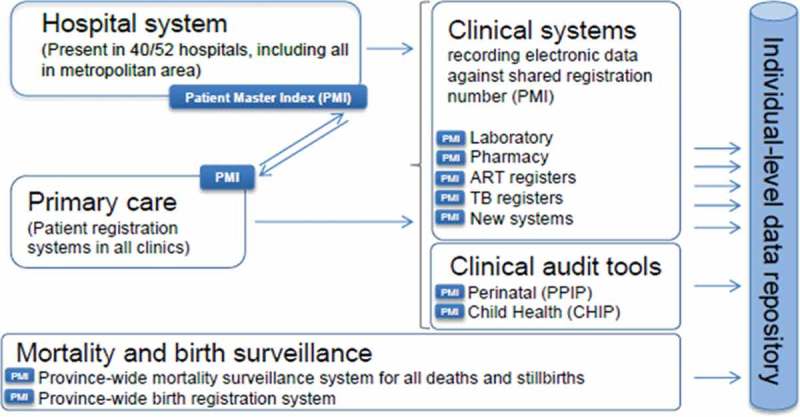
Introduction: To evaluate long-term outcomes in HIV-infected adolescents, it is important to identify ways of tracking outcomes after transfer to a different health facility. The Department of Health (DoH) in the Western Cape Province (WCP) of South Africa uses a single unique identifier for all patients across the health service platform. We examined adolescent outcomes after transfer by linking data from four International epidemiology Databases to Evaluate AIDS Southern Africa (IeDEA-SA) cohorts in the WCP with DoH data.
Methods: We included adolescents on antiretroviral therapy who transferred out of their original cohort from 10 to 19 years of age between 2004 and 2014. The DoH conducted the linkage separately for each cohort and linked anonymized data were then combined. The primary outcome was successful transfer defined as having a patient record at a facility other than the original facility after the transfer date. Secondary outcomes included the proportion of patients retained, with HIV-RNA <400 copies/ml and CD4 > 500 cells/µl at 1, 2 and 3 years post-transfer.
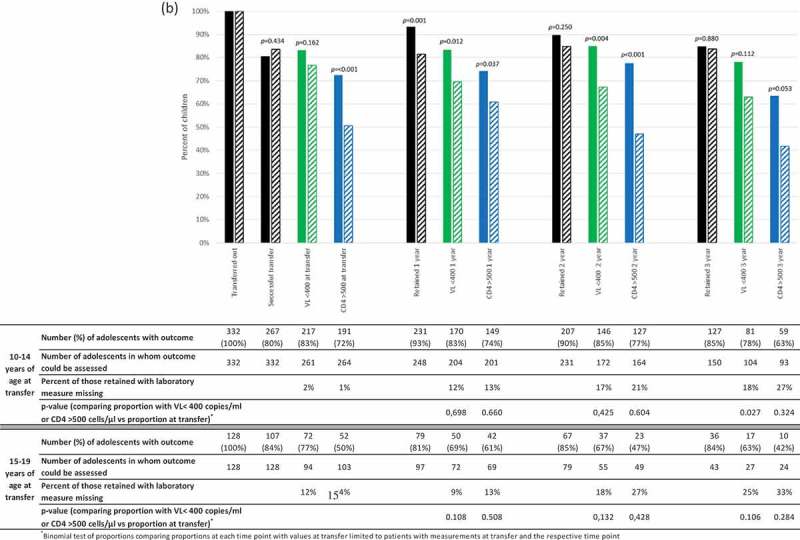
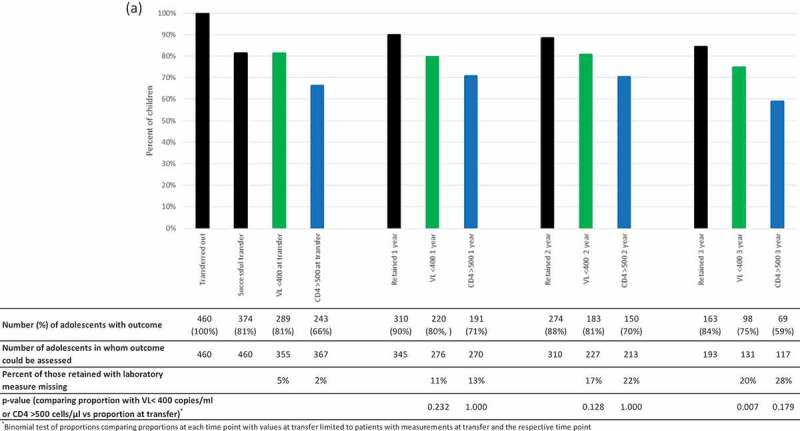
Results: Of 460 adolescents transferred out (53% female), 72% transferred at 10-14 years old, and 79% transferred out of tertiary facilities. Overall, 81% of patients transferred successfully at a median (interquartile range) of 56 (27-134) days following transfer date; 95% reached the transfer site <18 months after transfer out. Among those transferring successfully, the proportion retained decreased from 1 to 3 years post-transfer (90-84%). There was no significant difference between transfer and 1-3 years post-transfer in the proportion of retained adolescents with HIV-RNA <400 copies/ml and CD4 > 500 cells/µl except for HIV-RNA <400 copies/ml at 3 years (86% vs. 75%; p = 0.007). The proportion virologically suppressed and with CD4 > 500 cells/µl was significantly lower at 1 and 2 years post-transfer in those transferring at 15-19 vs. 10-14 years of age. Using laboratory data alone over-estimated time to successful transfer.
Conclusions: Linking cohort data to health information system data allowed efficient assessment of post-transfer outcomes. Although >80% of adolescents transferred successfully with nearly 85% of them retained for 3 years post-transfer, the decline in the proportion virologically suppressed and poorer outcomes in older adolescents are concerns..
Keywords: HIV-1; adolescents; antiretroviral; data linkage; sub-Saharan Africa; transfer; transition.
Conflict of interest statement
All authors have no conflicts of interest to declare.
Figures
References
-
- UNAIDS AIDSinfo Online Database [cited 2016. July 1]. Available from http://www.aidsinfoonline.org/devinfo/libraries/aspx/Home.aspx
-
- Johnson L, Davies M, Moultrie H, Sherman G, Bland R, Rehle T, et al. The effect of early initiation of antiretroviral treatment in infants on pediatric AIDS mortality in South Africa - A model-based analysis. Pediatr Infect Dis J. 2012;31:474–24. - PubMed
-
- Maskew M, Bor J, MacLeod W, Carmona S, Sherman G, Fox MP.. The youth treatment bulge in South Africa: increasing numbers, inferior outcomes among adolescents on ART. International AIDS Conference Durban South Africa; 2016.
MeSH terms
Substances
Grants and funding
- Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD)/International
- 1R21HD089859-01/HD/NICHD NIH HHS/United States
- R21 HD089859/HD/NICHD NIH HHS/United States
- 3U01AI069924-11/National Institute of Allergy and Infectious Diseases/International
- U01 AI069924/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
